External Ophthalmomyiasis Caused by Oestrus ovis: A Rare Case Report from India
Article information
Abstract
Myiasis of different organs has been reported off and on from various regions in the world. We report a human case of external ophthalmomyiasis caused by the larvae of a sheep nasal botfly, Oestrus ovis, for the first time from Meerut city in Western Uttar Pradesh, India. A 25-year-old farmer presented with severe symptoms of conjunctivitis. The larvae, 3 in number, were observed in the bulbar conjunctiva, and following removal the symptoms of eye inflammation improved within a few hours.
INTRODUCTION
Myiasis is infection of tissues or organs of animals or man by larvae of a fly. The common sites are skin wounds. Eyes, nose, nasal sinuses, throat, and urogenital tract are less common sites [1-3]. Ocular involvement occurs in about < 5% of all cases of human myiasis [4]. Ophthalmomyiasis is classified as ophthalmomyiasis externa if the larvae are present on the conjunctiva, and ophthalmomyiasis interna when there is intraocular penetration of larvae [5]. Cases of ophthalmomyiasis externa have been reported from various parts of the world [6-8]. However, this condition is rare in India and there are only a few reported cases [5,9-12]. To the best of our knowledge, no case of ophthalmomyiasis externa caused by Oestrus ovis (the sheep nasal botfly) has been reported from this part of India. The present case therefore highlights the awareness among the ophthalmologists regarding larval conjunctivitis in spring and summer season, with timely diagnosis and treatment of this rather rare infestation.
CASE REPORT
A 25-year-old male farmer came to our outpatient department in April 2008 with a 2-day history of foreign body sensation, burning, and excessive watering from his right eye. He gave a history of something falling in his eye while he was resting below a tree after lunch in the field. He was absolutely fine before that, and there was no significant history of ocular or medical problems preceding this.
On examination it was found that his visual acuity was 20/20 in both eyes. Eyelids of the affected right eye were absolutely normal. The conjunctiva was mildly congested with profuse lacrimation. Extraocular movements were full. On slit lamp examination, the most remarkable finding was the presence of tiny translucent worms, 1-2 mm in size with dark heads, crawling over the bulbar conjunctiva and cornea. The larvae actively avoided the bright light of the slit lamp and tried to burrow deep into the conjunctival fornices. Pupillary reaction was normal. Slit lamp examination did not reveal any anomaly. Using a topical anesthesia with 4% xylocaine drops these larvae were allowed to crawl on the sterile cotton swab sticks placed over the conjunctiva. The larvae (3 in number) were mounted on a glass slide and sent to department of microbiology for identification.
Direct and indirect ophthalmoscopy showed no evidence of intraocular organisms or inflammation. Examination of his left eye was normal. Topical antihistaminic and antibiotic drops were prescribed. When the patient came for a follow-up 2 days later, he was completely relieved of his symptoms of foreign body sensation and excessive watering. A repeat slit lamp examination of the anterior segment and fundus was normal. The larvae mounted on a microscopic slide were examined carefully and photographed under a microscope. It was identified as the first stage larvae of O. ovis, which is a larviparous dipteran on the basis of their spindle shaped skeleton (Fig. 1). The larvae also showed a pair of sharp dark brown oral hooks and tufts of numerous brown hooks on the anterior margin of each body segment (Fig. 1). The posterior spiracles were found, in the eighth segment [12].
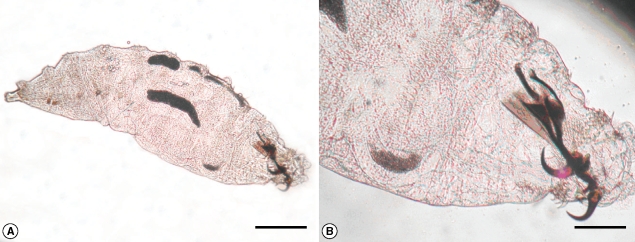
A wet mount showing the spindle shaped skeleton (A) and dark brown oral hooks (B) of an Oestrus ovis larva extracted from the patient. Scale bars = 0.5 mm (A) and 0.2 mm (B).
DISCUSSION
The sheep nasal botfly, O. ovis, are large dark gray flies with dark spots on the dorsum of the thorax and abdomen, and are covered by a moderate amount of light brown hair [13]. Although myiasis in man is generally rare, members of the Oestridae (Diptera) may produce human myiasis in countries where the standard of hygiene is low and there is abundance of flies around the locality [8]. The female sheep nasal botfly dashes to deposit their freshly hatched larvae in the naris, on the conjunctiva, on the lip, and in the mouth of the usual hosts like sheep, cattle, and horse. Man serves as an accidental host [13].
Opthalmomyiasis due to O. ovis was described for the first time in 1947 by James [8]. External ophthalmomyiasis manifests as acute catarrhal conjunctivitis with symptoms similar to those presented in this case [1]. Therefore, ophthalmomyiasis externa caused by O. ovis should not be regarded as a benign condition and should be treated promptly to prevent serious complication such as corneal ulcer, decreased vision, and invasion into eye globe causing endophthalmitis, iridocyclitis, and even blindness which has been reported in the past [14]. However, none of these complications were encountered in our patient. It may have been due to a small number of larvae, i.e., only 3 in our case, and a short history of 2 day duration.
Our patient came in April (the spring season). A previous paper presenting clinical manifestations and seasonal variations of 8 ophthalmomyiasis cases have reported that most of them occurred in the spring and summer seasons [1]. The present case highlights 2 things first, it creates awareness among the ophthalmologists regarding larval conjunctivitis as 1 of the causes of conjunctivitis during the spring and summer seasons especially in developing countries like India, where the general standard of hygiene is low and there are a large number of flies around. Second, irrigation of the conjunctiva with normal saline is unsuccessful in washing out the larvae because the larvae grab the conjunctiva firmly with the help of a pair of oral hooks and numerous hooks on each segment. Therefore, after anesthetizing the conjunctiva, a thorough examination of the eye under magnification and prompt removal of the larvae manually with sterile cotton swab sticks should be done to avoid disastrous complications of internal ophthalmomyiasis.