Opportunistic Parasites among Immunosuppressed Children in Minia District, Egypt
Article information
Abstract
A total of 450 stool samples were collected from inpatient and outpatient clinics of Pediatric Department, Minia University Hospital, Minia District, Egypt. Two groups of patients were studied, including 200 immunosuppressed and 250 immunocompetent children. Stool samples were subjected to wet saline and iodine mounts. A concentration technique (formol-ether sedimentation method) was carried out for stool samples diagnosed negative by wet saline and iodine mounts. Samples were stained by 2 different methods; acid fast stain (modified Ziehl-Neelsen stain) and Giemsa stain. Total 188 cases (94%) were diagnosed positive for parasitic infections among immunosuppressed children, whereas 150 cases (60%) were positive in immunocompetent children (P<0.0001). The most common protozoan infection in immunosuppressed group was Cryptosporidium parvum (60.2%), followed by Blastocystis hominis (12.1%), Isospora belli (9.7%), and Cyclospora caytenensis (7.8%). On the other hand, Entamoeba histolytica (24.6%) and Giardia lamblia (17.6%) were more common than other protozoans in immunocompetent children.
INTRODUCTION
Opportunistic infections are infections with a facultative pathogenic organism. This infection uses human beings not only for a host but also for multiplication. Serious pathological changes are uncommon in immunocompetent hosts as long as the human immune system is functioning normally [1]. The intracellular intestinal protozoan Cryptosporidium parvum, Cyclospora cayetanensis, Isospora belli, and Blastocystis hominis are the major causes of uncontrollable debilitating diarrhea in developing countries [2]. The infection is self-limiting in immunocompetent hosts, which readily clear the parasites, but it may cause persistent diarrhea and severe malabsorption in immunodeficient hosts [3].
Other kinds of parasites, such as Entamoeba histolytica, Giardia lamblia, Trichuris trichiura, Ascaris lumbricoides, Strongyloides stercoralis, and hookworms are also frequently encountered in developing countries [4]. These parasites are often the cause of self-limiting diarrhea [4]. However, S. stercoralis is frequently detected in immunosuppressed patients; the parasite multiplies in the human host by means of autoinfection [5].
The relationship between immune status and the presence of intestinal parasites in Minia District, Egypt has not been studied. Therefore, this work was designed to detect the frequency and distribution of intestinal opportunistic parasites among immunocompetent and immunosuppressed children.
MATERIALS AND METHODS
Subjects and methods
This is a cross sectional study where a total of 450 cases who complained of chronic diarrhea (minimum of 3 loose stools per day with a duration of more than 2 weeks) had been collected from inpatient and outpatient clinics of Pediatric Department of University Hospital, Minia District, Egypt after their oral acceptance to be enrolled in this study. The first group was composed of 200 patients who had immunocompromising underlying disorders; 60 cases (30%) with severe malnutrition, 50 cases (25%) with chronic diseases, 65 cases (32.5%) were receiving corticosteroids, and 25 cases (12.5%) with malignancies. The immunodeficiency status was confirmed by certain investigations (% of lymphocytes among leucocytes and CD4+ T-cell count). The second group consisted of 250 patients who were without any evidence of immunodeficiency symptoms. Diarrhea is generally associated with other signs suggesting enteric involvements, including nausea, vomiting, abdominal pain, fever, passage of bloody stools (dysentery), and tenesmus.
A clean, plastic container was given to each person. One stool sample per subject was collected. All information, including personal identification, the stage of disease, and clinical symptoms were recorded. Fecal specimens were transported to the Parasitology Laboratory, College of Medicine, Minia University to be examined by different techniques for parasitic infections within 1-3 hr of collection.
Stool examinations
Macroscopic examinations
This examination was done for identifying the followings: color and smell of the stool, presence of blood and mucus, presence of round worms, thread worms, or tapeworm proglottids, and consistency. The consistency of the stool could be classified as formed, soft, loose, or watery. The cysts were found maximally in the formed stool while trophozoites were most abundant in watery stool.
Microscopic examination
Direct wet smear methods, namely saline wet mount and iodine wet mount were applied:
(1) Saline wet mount: It was used to detect worm eggs or larvae, protozoan trophozoites, and cysts. In addition, it could reveal the presence of RBCs and WBCs.
(2) Iodine wet mount: This was used to stain glycogen and nuclei of protozoan cysts.
Concentration technique was used when the number of parasites in the stool specimens was low by a direct wet mount. Eggs, cysts, and larvae could be recovered after concentration procedures whereas trophozoites were destroyed during the procedure. This was why direct wet mount examination was used at the initial phase of microscopic examinations. The concentration procedure (formol-ether sedimentation method) was done according Dubey et al. [6], in which the eggs and cysts settle down at the bottom.
Fixation and smear preparations
A small amount of stool (25 g) was mixed with 10 ml of fixation buffer and incubated for 1 hr to be fixed and inactivated. The suspension was passed through 4 layers of netting cotton and centrifuged at 2,000 g for 5 min. Three smears were made from the pellet, dried in air, fixed with methanol and/or acetone, and then examined using 2 different stains; acid fast stain (modified Ziehl-Neelsen stain) according to El-Shazly et al. [7] and Giemsa stain according to Garcia [8].
Stool culture for nematode larvae
Stool samples were cultured on agar plates for detection of S. stercoralis or hookworm larvae. Agar plates were freshly prepared every evening, and stored at 4℃. A groundnut-sized portion of a stool sample (~2 g) was placed in the middle of the agar plate. The closed Petri dish was incubated in a humid chamber for 2 days at ambient temperature. Following incubation, the plates were examined for the presence of S. stercoralis and hookworm larvae under a light microscope. The larvae of hookworms were usually more inert and tended to stay closer to where the stool sample had been placed on the agar, whereas S. stercoralis larvae are more active and mobile. However, discriminative characteristics can only be determined under a microscope. Hence, the plates were rinsed with 10 ml of a 10% acetyl-formalin solution. The eluent was centrifuged at 500 g for 1 min, and the sediment was microscopically examined at 400× magnification. Hookworms and S. stercoralis were determined on the basis of established morphologic characteristics, i.e., the long buccal cavity and small genital primordium of hookworm larvae, and the short buccal cavity and large genital primordium of rhabditiform (L1) S. stercoralis larvae. The filariform larvae (L3) of the latter nematode can be identified by their characteristic forked tail [9].
Statistical analysis
Data were coded and verified prior to data entry. The Statistical Package of SPSS version 16 for windows was used for data entry and analysis. Descriptive statistics were calculated. For qualitative data, χ2-test was used, and z-test was used for proportions. A significant P-value was considered when it was less than 0.05.
RESULTS
Percentage of opportunistic infections among studied individuals
Total 188 cases (94%) were diagnosed as positive for parasitic infections among immunosuppressed patients, whereas 150 cases (60%) were positive among immunocompetent patients. This difference was statistically significant (P<0.0001).
Influence of different detection methods on detection of parasitic infections
We investigated various techniques for detection of parasites. Examination of the stool samples revealed that 320 out of 450 samples (71%) were confirmed positive for parasitic infections by wet saline technique. However, this incidence increased to 338 (75.1%) when the concentration method and stained method were used (Table 1).

Positivity of opportunistic infections by different examination techniques
Relationship between type of parasitic infections and immune status of children
Comparison of the 2 studied groups showed that protozoal infection was higher among the immunosuppressed group than the immunocompetent group. These data was statistically insignificant (53.9% vs 46.1%; P=0.07). On the other hand, helminth infections were significantly higher among the immunosuppressed group than the immunocompetent group (73.3% vs 26.7%; P=0.0001). Among different protozoal infections, C. parvum was the most common species both in the immunosuppressed and immunocompetent children, followed by B. hominis, then I. belli, and finally C. caytenensis (Table 2). The detected stages of these protozoa are shown in Fig. 1. On the other hand, the incidence of E. histolytica and G. lamblia were more common in the immunocompetent children than in the immunosuppressed children (Table 2). The different kinds of helminths detected in this study are shown in Table 3. The detected stages of these helminths are shown in Fig. 2.

Percentage of protozoan infections between immunosuppressed and immunocompetent patients
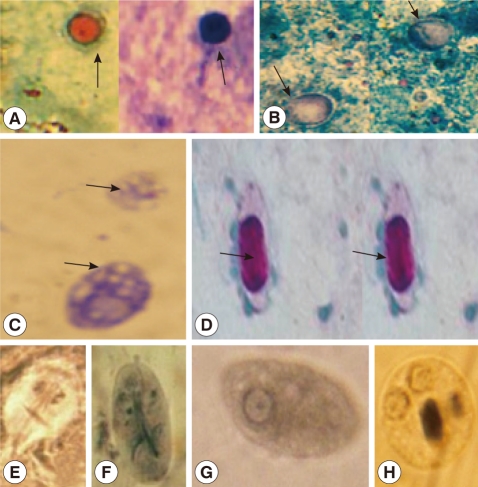
Size, shape, and overall morphologic features of the protozoa identified using a modified acid-fast stain and also Giemsa stain (oil; ×1,000). (A) Cryptosporidium parvum oocysts, 4 to 6 µm in diameter, and round to irregular in shape. The oocysts are stained red with modified acid-fast stain and stained blue with Giemsa stain. (B) The oocysts of Cyclospora cayetanensis, 7.7 to 10.0 µm in diameter. The oocysts stained bright pink with modified acid-fast stain. (C) The oocysts of Blastocystis hominis, 6 to 8 µm in diameter, and round to irregular in shape. They have multiple vacuoles and dark thin peripheral layer of cytoplasm in multivacuolated form. The oocysts stained blue with Giemsa. (D) Isospora belli demonstrates the characteristic large, thick-walled immature oocyst containing the modified acid-fast sporoblast. The oocysts of I. belli, 20-33×10-19 µm. (E) Trophozoite of Giardia lamblia in oval or pear-shape, 9-21×5-15 µm. It has 4 flagella and 2 oval nuclei located anterior in a sucking disk. (F) Cyst of G. lamblia oval in shape, and measures 8 to 12 µm in length. The cytoplasm is retracted from the cyst wall and has 4 nuclei at 1 pole. (G) Trophozoite of Entamoeba histolytica in irregular shape, 15 to 40 µm in diameter. It has a nucleus with thin nuclear membrane, central karyosome, and fine peripheral chromatin regularly arranged on nuclear membrane. (H) Cyst of E. histolytica, binucleated, 10 to 20 µm in diameter.

Percentage of intestinal helminths between immunosuppressed and immunocompetent children

Size, shape, and overall morphologic features of the detected stages of the helminths (×400). (A) Egg of Taenia spp. It is rounded with thick-brown radially striated wall and contain mature embryo, 30 to 40 µm in diameter. (B) Egg of Hymenolepis nana. It is ovoid, translucent, mature, and characterized by the presence of polar filaments, 70-85×60-80 µm in diameter. (C) Egg of Ascaris lumbricoides. It is fertilized egg, Oval and brown. It has a coarse albuminous lamillated layer and is immature (contains 1 cell stage), 50-90 µm in diameter. (D) Egg of Enterobius vermicularis. It is translucent in color and D-shaped. It is mature (contain fully developed larva), and 140-150 µm in length. (E) Rhabditiform larvae of Strongyloides stercoralis; the first stage larva (L1). It has short buccal cavity, blunt tail end, and a large genital primordium, and its esophagus is rhabditiform, 0.3 mm long. (F) Adult male of Strongyloides stercoralis, 0.7 mm in length. It has rhabditifrom oesophagus. The posterior end is curved ventrally with 2 short (arrow).
Influence of cause of immunosuppression on the positivity of opportunistic infections
The cause and the degree of immunodeficiency are shown in Table 4. Children with chronic diseases and those with severe malnutrition showed higher frequencies of protozoal infections than those chronically treated with corticosteroids and those who had malignancy (98% and 96.7% vs 92.3% and 84%, respectively). C. parvum was the most common organism among those with severe malnutrition and those with chronic diseases (77.6% and 61.2%, respectively). B. hominis was found in 22.4% and 10.2% of the same groups of patients. C. parvum was found in 33.3% and 23.8% of patients who were chronically treated with corticosteroids and those who had malignancies, respectively. B. hominis was found in 1.7% and 4.8% of the same groups of patients.

Comparison between immunosuppressed and immunocompetent children with regard to the immune status
DISCUSSION
C. parvum, B. hominis, and I. belli were consistently found in immunosuppressed patients with chronic diarrhea [4]. However, these opportunistic parasites were rare in immunocompetent patients [10]. In the present study, we also found that the frequency of protozoal infections among immunosuppressed children was significantly higher than that of immunocompetent children.
Fontanet et al. [11] found that the prevalence of intestinal parasites in immunosuppressed patients was as same as that in immunocompetent individuals. The present study found that cryptosporidiosis was the most common protozoa in both groups; however, the prevalence was higher in immunosuppresed group (60.2% vs 42.2%). This could be explained by that reduction in local and cell-mediated responses to intestinal parasites in immunosuppressed patients may selectively favor the establishment of some organisms [5]. These data were in agreement with the results obtained by Ribes et al. [12] who found that C. parvum produces diarrheal syndromes with profuse, watery diarrhea, and the disease manifestations tend to be more severe and protracted and more common in immunocompromised patients, in whom it can produce extreme weight loss and wasting [12]. However, Oshiro et al. [13] found that there was no connection between the presence of C. parvum and diarrhea [13].
The current study found that B. hominis infection was positive in 12.1% of immunosuppressed patients and in 7.2% of immunocompetent patients. This was in agreement with the findings obtained by Escobedo and Nunez [14]. It has been reported that patients with suppressed immunity and positive for B. hominis infection were presented with diarrhea and other gastrointestinal symptoms [8,15]. Moreover, I. belli was detected in 9.1% of immunosuppressed patients and in 6.3% of immunocompetent patients. This data was in agreement with many other studies [15,16].
On the other hand, intestinal protozoans E. histolytica and G. lamblia were more prevalent in patients with immunocompetent status than in immunosuppressed status (24.6% vs 6% and 17.6% vs 4.8%, respectively). These results could be explained by that infection in immunosuppressed patients may cause some changes in the gut structure that may not be suitable for E. histolytica and G. lamblia.
However, the reasons for these patterns in parasite distribution are unclear. It had been postulated that colonization of the intestinal tract by parasites might be influenced by enteropathy induced by any causes that make suppression of the immunity. Also, this may selectively determine the establishment and/or survival of extracellular and luminal parasites. In contrast, whereas the gut of immunosuppressed individuals may not be a favorable environment for the establishment and/or survival of extracellular parasites, the mucosal dwelling organisms may not be adversely affected by the pathologic changes [5].
With regard to helminths, S. stercoralis is frequently detected as an intestinal parasite in immunosuppressed than in immunocompetent diarrheal patients. Non-opportunistic helminths, including Ascaris lumbricoides, Entrobius vermicularis, and hookworms, were frequently encountered in developing countries [4]. However, in our study, we detected small numbers of infected children with these helminths either in immunosuppressed or immunocompetent groups with no significant difference observed between the groups (P>0.7).
ACKNOWLEDGMENTS
The authors would like to thank Professor Nabil Shokrany Gabr, Head of the Department of Parasitology, Faculty of Medicine, Minia University for his continuous advices through the technical procedures. Thanks are extended to Professor Nawras M. Mowafy, Department of Parasitology, Faculty of Medicine, Minia University for her guiding us through the technical intricacies as well as writing this paper. The authors would also like to thank Professor Rafaat M. Khalifa, Department of Parasitology, Faculty of Medicine, Assuit University his continuous advices.