Analysis of vivax malaria cases in Gangwon-do (Province), Korea in the year 2000
Article information
Abstract
A total of 827 malaria cases were reported in the Gangwon-do in the year 2000. There were 18.2 cases per 100,000 inhabitants. There were 283 cases among civilians and 544 cases among the military. 90.6% of cases were reported in Cheorwon- (531), Hwacheon- (152), and Goseong- (66) gun (county), which bordered the demilitarized zone (DMZ). A distinct feature pertaining to the malaria cases in Gangwon-do is that the number of cases has increased about two times over the last year. The mean time from the beginning of symptoms to malaria diagnosis was five days. Control systems for malaria by public health organizations and military organizations are well maintained, but were not able to reduce the malaria prevalence rate. The cause for the increase in pattern of the malaria cases in Gangwon-do may be caused by the spreading of prevalent areas of malaria to the east. Continuous endeavor such as early detection of cases, early treatment, education on clinical symptoms and prevention of mosquito bites with repellent and mosquito nets will help to reduce the infection rate of malaria in Gangwon-do.
INTRODUCTION
Since the first military case of tertian malaria infection in Paju in 1993 (Chai et al., 1994), 107 cases in 1995, 356 cases in 1996, and 1,724 cases in 1997 have been reported (National Institude of Health, Korea, 1996, 1997, 1998; Kho et al., 1999). More than 3,000 cases of malaria infections were reported in 1998 (Chai, 1999), and the areas in which infections have been reported to spread to most parts of the country. The total number of malaria cases in 1999 was lower than in 1998. However, the civilian cases were higher than those of the military.
Most of the malaria cases are soldiers, discharged soldiers, or civilians living in 13 different areas. They were the counties of Yeoncheon, Gangwha, Pocheon, Ongjin, Yangju, Yanggu, Hwacheon and Cheorwon, the cities of Paju, Gimpo, Dongducheon, Goyang, Uijeongbu in Gyeonggi-do, Incheon, and Gangwon-do bordering the DMZ. The areas showed more than 10 cases of malaria infections per 100,000 inhabitants (National Institude of Health, Korea, 2000). According to the limited data of the malaria infection in September of 2000 (National Institute of Health, Korea. 2000), we found that the incidence of cases was greater than that of 1999 and different from the result of Gyeonggi-do and Incheon. Cases among soldiers were also increased in the Gangwon-do, but the ratio of malaria cases between soldiers and civilians was decreased in Gyeonggi-do (National Institute of Health, Korea, 2000). The number of cases in the Gangwon-do, make this area a high epidemic region, therefore an analysis of infection state and control programs is necessary. Thus, the main purpose of this survey is to provide epidemiologic data pertaining to malaria control in Gangwon-do.
MATERIALS AND METHODS
Data sheets of the civilian cases were collected at public health centers. Data in this survey were confined to cases in Gangwon-do in the year 2000. We used a data sheet written for each case of the civilians. The contents of the sheets were 1) occupation, 2) clinical symptoms, 3) duration of symptoms, 4) visit in relation to onset of the symptoms, 5) past history of malaria infection, 6) environmental situation of patients related to malaria, 7) military service, 8) drug intake for prevention of malaria during military service, 9) travel experience, and 10) donation of blood and blood transfusions. The soldiers who did military service in Gangwon-do were surveyed on the military service areas that existed until December of 2000 and on the developing time of the symptoms. We used the data of the National Institute of Health on malaria control and management in the military. There were confirmed 827 cases of malaria infection including 283 civilian and 544 soldier cases.
RESULTS
There were 827 cases of confirmed malaria infection in Gangwon-do in the year 2000. Of these 283 were civilian cases and the remaining 544 cases were soldiers, and 90.6% of them were reported in Cheorwon-, Hwacheon- and Goseong-gun which border the DMZ (Table 1).

Malaria cases of Gangwon-do by residence in 2000
Civilian
For civilian cases there were 18.2 malaria cases per 100,000 inhabitants. Among these cases, there were 164 (58%) males and 119 (42%) females. By age group, malaria cases of the people in their fifties were most prevalent at 38.3 cases per 100,000 inhabitants (Fig. 1). There were 87 (30.9%) cases among people who are under the age of 30 years old and 19 (6.7%) in those who are over 70 years old. Considering the areas that border the DMZ and other areas of the country, it was found that for cases over 40 years of age the rate was 64% and for those under the 40 years of age was 36% in DMZ border areas. For cases under the age of 40 years the rate was 66.3% in other areas. There was one relapse case in the past three years, in which 70% of the cases were living in the DMZ border area. Another suspected cause of infection was military service in DMZ border areas (11%), blood transfusion in the past three years (8.8%), and travel to DMZ border areas (5.7%). Among the three cases, 13.4% had a malaria history in their family or neighbors.
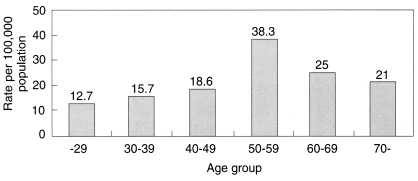
Malaria incidence in Gangwon Province by age group in 2000.
In the occupational distributions of civilian cases, there were 112 cases in farmers and housekeeping was next at 49 cases (Fig. 2)

Occupational distribution of the civilian malaria cases in 2000.
There were no reported cases in Yeongwol until the year 2000 and the first cases were confirmed in Inje, Donghae, Pyeongchang, and Hongcheon in 2000 (Table 2). Early symptoms of these cases were fever (90.8%), chills (90.5%), headache (83.4%), fever and chills (66.4%). myalgia (66.4%), diarrhea (10.6%), and cough (12.7%). 88% of the cases were diagnosed within 10 days from the first symptoms and the mean time for the diagnosis was 5 days (Fig. 3).
Regional distributions of civilian malaria cases from 1997 to 2000 in Gangwon-do
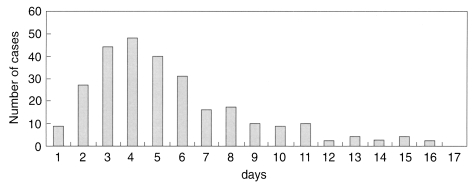
The time required for confirmation of malaria after the onset of clinical manifestation in civilian cases.
Military
In the 544 malaria cases among the military, Cheorwon had 366 cases, Hwacheon had 94 cases, Goseong had 55 cases, and there was no cases in Gangneung. In the monthly prevalence of the cases in the military, there were no cases in January, February and December (Table 3).
Malaria cases of Gangwon-do population by month in 2000
DISCUSSION
Frequent malaria infections in soldiers and civilians were confirmed in Cheorwon, Hwacheon and Goseong that border the DMZ in the eastern parts of Korea. Distribution of civilian malaria cases in the DMZ border area such as Cheorwon, Hwacheon, Goseong, and Gangneung were 165, 12, 11, and 58 cases respectively. This showed that these areas had higher incidences than any other areas of Gangwon-do. Most of the cases in Cheorwon lived within 12 km of the DMZ and did agricultural works. Areas in Gangwon-do showed an increasing pattern of malaria infections compared to last year. Few civilian cases who were confirmed with malaria were not inhabitants of Gangwon-do, but they were counted as cases in Gangwon-do, because they got the Infection while they stayed in Gangwon-do.
Areas that bordered the DMZ from the West in Gangwon-do are Cheorwon, Hwacheon, Yanggu, Inje and Goseong. Only 2 cases were reported in Yanggu and Inje, but 11 cases were reported in Goseong which is located in the most eastern part. Most of the areas in Yanggu and Inje are mountains, so it is difficult for the mosquitos to develop. Goseong has lakes and fields over the DMZ, so it provides good conditions for mosquitoes. Cheorwon showed the most cases of infection, because they border the DMZ and had the largest agricultural area and the biggest proportion of agricultural area to the total area (Gangwondo, 1999). Therefore, the behavior of the farmers and environmental factors may influence the rate of the malaria infections. Gangneung had 12 cases of malaria in the year 2000. Gangneung does not border the DMZ, but had 2 malaria cases in 1999. All of the cases were male and 11 cases were retired soldiers who had military service in Gyeonggi- and Gangwon-do that bordered the DMZ.
Civilian cases in the fifties showed 38.3 cases per 100,000 inhabitants and incidences as high as 59 (21%) in any age group. Civilians of older age living around the DMZ is associated with the result. There were 87 (30.9%) cases under the civilians 30 years of age and they had a history of travel, military service, and other history of visiting malaria prevalent areas. Cases over 40 years of age accounted for 64% of cases in DMZ bordering areas but only 33.7% in other areas. This result suggests that the cases in people who live in non-bordering areas were probably caused by travel or military service in these areas.
Only one relapse case was reported and 70% of the cases were living in the DMZ bordering areas. Other suspected causes of infection were the experience of military service in DMZ border areas (11%), blood transfusion in the past three years (8.8%), and travel to the DMZ border areas (5.7%). It is hard to know the exact cause of malaria infections among those who had several reasonable infection factors. We suspect the route of malaria infection to the non-border areas of the DMZ is from military service and travel to the DMZ area. Some of the malaria cases are suspected to be from blood transfusions.
The time required for diagnosis was 23.6 days in 1995, 13.7 days in 1997, 11 days in 1999, and 5 days in the year 2000 (Lee et al., 1998; National Institute of Health, Korea, 2000). Shortening of the diagnostic period resulted from the help of public health programs. Most of the regional health organizations in Gangwon-do promoted malaria control. These included committee organization for regional malaria control, density study of mosquitos, education of workers in public health administration, public information to civilians, and support with drugs for prevention of malaria (National Institute of Health. Korea, 2000). Several inadequacies, such as lack of a relationship with a specialist on malaria, lack of cooperation with military, and insufficient budget for malaria control were revealed during the malaria control study in Gangwon-do in 2000.
Despite the malaria control endeavor by military organization, there were 544 malaria cases in the year 2000 and increased by almost two folds compared to the 293 cases in 1999 (National Institute of Health, Korea, 2000). If there were no efforts to control malaria infections by the military, the number of malaria cases in soldiers would be higher than the result shown in this study. In the 544 malaria cases in the military, there were no cases in Gangneung. This made it different from the civilian cases. But many of the civilian cases in Gangneung were retired soldiers who did military service in DMZ or DMZ bordering areas. The results between military and civilian cases showed no significant difference. The causative factor was the regional factor for both soldiers and civilians. The infection pattern of the military cases showed a similar pattern to civilian cases, but there were no cases in January, February, and December. In civilians, some of the cases were detected in March and April of 2000, but none in 1999.
The flowing down of infected mosquitoes flying from the northern part of the DMZ to the South area is strongly suspected (Chai, 1999; Lee et al., 2001). It is expected that the mosquitoes will bite soldiers and civilians. The goal of malaria control in Gangwon-do is to reduce the malaria cases, prevent the dispersion of mosquitoes, and induce malaria eradication. The malaria prevalent area is around the DMZ and its bordering areas, so there is a need to work cooperatively with the DPRK to approach this goal. One of the effective malaria control methods is to prevent bites by mosquitoes, which are infected with malaria. It was reported that malaria in Korea was in an unstable state and it would not be possible for it to be endemic in South Korea judging from epidemiological and socio-ecological factors (Lee, 2000).
There has been many donations of blood by soldiers serving in malaria prevalent areas in the Gangwon-do (Lim et al., 1997; Jeong et al., 1999). Improved management of blood transfusion and blood product is needed. It was reported that malaria transmission by Anopheles sinensis resulted from high population density, but not high transmission potential (Lee et al., 2001). For this reason, inhabitants living in malaria prevalent areas in Gangwon-do should do their best to decrease vector population and prevent mosquito bites. Early detection and treatment, public education on malaria for inhabitants and travelers, and management of soldiers who serve in DMZ bordering areas will help to control malaria in Gangwon-do.