Abstract
Knowledge of the prevalence of human Toxoplasma gondii infection is required in the Republic of Korea. In this study, we surveyed the seroprevalence of T. gondii infection and analyzed the risk factors associated with seropositivity among residents in 2 administrative districts; Seoul and the island of Jeju-do, which have contrasting epidemiologic characteristics. Sera and blood collected from 2,150 residents (1,114 in Seoul and 1,036 in Jeju-do) were checked for IgG antibody titers using ELISA and for the T. gondii B1 gene using PCR. In addition, participants completed a questionnaire that solicited information on gender, age, occupation, eating habits, history of contact with animals, and travel abroad. The T. gondii B1 gene was not detected in all residents examined. However, ELISA showed 8.0% (89 of 1,114 sera) positive for IgG antibodies against T. gondii in Seoul and 11.3% (117 of 1,036 sera) in Jeju-do. In both districts, the positive rates were higher in males than in females, and those 40-79 years of age showed higher rates than other ages. In Seoul, residents older than 70 years of age showed the highest positive rate, 14.9%, whereas in Jeju-do the highest prevalence, 15.6%, was in those in their sixties. The higher seropositive rate in Jeju-do than in Seoul may be related to eating habits and occupations. The present results and a review of related literature are indicative of an increased seroprevalence of T. gondii in Korea in recent years.
-
Key words: Toxoplasma gondii, seroprevalence, B1 gene, resident, Seoul, Jeju-do, IgG, ELISA
INTRODUCTION
Toxoplasma gondii, a coccidian protozoan, is distributed worldwide. This intracellular protozoan can infect essentially all nucleated eukaryotic cells of warm-blooded animals, including humans and vertebrate animals, and can cause clinical manifestations, such as lymphadenitis, encephalitis, retinochoroiditis, congenital infection, and neonatal mortality [
1-
3]. Transmission to humans occurs through ingestion of
T. gondii bradyzoites or tachyzoites contained in undercooked meat of infected animals or ingestion of oocysts originating from the feces of infected cats [
1-
3]. Transplacental infection from mother-to-fetus is also well known [
4]. In immunocompetent individuals,
T. gondii infection is usually asymptomatic or causes only mild symptoms [
1-
3,
5]. However, it can elicit severe clinical manifestations in immunocompromised conditions, including AIDS, transplantation, malignant disease, and pregnancy [
5]. Congenital toxoplasmosis may cause stillbirth, abortion, or other serious damages to the fetus, such as meningoencephalitis and hydrocephalus [
4,
5].
In the Republic of Korea (hereafter referred to as Korea), the seroprevalence of toxoplasmosis has been studied by many researchers [
6-
23]. From 1960 until 1999, residents, children, and hospital patients in Korea usually showed relatively lower prevalences, ranging from 1.1-7.7%, compared to American and European locales [
3,
5,
6-
13]. However, from 2000-2009, the seroprevalence of toxoplasmosis showed a tendency of slight increase [
14-
20]. In particular, the prevalence on Jeju-do Island (hereafter referred to as Jeju-do) among an adult population was reported as 12.9% [
14]. Thereafter, the reported seroprevalence in Korean residents have been, with the exception of one report [
21], higher than this figure, ranging from 13.2-25.8% [
22-
24]. In this respect, it has been assumed that the seroprevalence of toxoplasmosis in Korea is presently increasing, presumably due to an increased consumption of domestic or imported pork, or other animal meat at risk of
T. gondii infection [
23].
The present study was conducted to determine the seroprevalence of T. gondii among people residing in 2 districts, Seoul and Jeju-do, which have contrasting epidemiologic characteristics related to the parasite life cycle and transmission. In addition, in order to assess the current status and trend of toxoplasmosis, the literature reporting the seroprevalence of toxoplasmosis among Korean people is briefly reviewed.
MATERIALS AND METHODS
Subjects and sample collection
We collected sera and blood from 2,150 residents (1,114 in Seoul and 1,036 in Jeju-do; 12-95 years of age) from March to September 2011, during health check-up in the Eastern Seoul, Western Seoul, and Jeju-do branches of the Korea Association of Health Promotion (KAHP). The sera and blood were stored at -80℃ until analyzed. This study was approved under the regulations established by the Institutional Review Board Committees of Seoul National University Hospital (No. C-1101-064-348, 17 April 2011), and KAHP (No. 11-C-02, 22 March 2011). Informed consent was obtained from each individual.
Preparation of T. gondii lysate antigen
Tachyzoites of T. gondii (RH strain) were collected from the peritoneal cavity of 6 week old BALB/c mice that had been previously injected 3-4 days before. The tachyzoites were washed 3 times with PBS and purified by centrifugation over 40% Percoll (Sigma-Aldrich, St. Louis, Missouri, USA). The tachyzoites were sonicated 5 times on ice and centrifuged at 100,000 g for 1 hr. The supernatant was collected for use as the soluble antigen. The protein content was measured using a Nanodrop 2000 spectrometer (Thermo Scientific, Wilmington, Delaware, USA).
ELISA to measure IgG titers
ELISA was performed as previously described [
11] with slight modifications. Briefly, 200 µl of
T. gondii lysate antigen (TLA) (5 µg/ml) in 0.05 M carbonate-bicarbonate buffer (pH 9.6) was coated on each well of a 96-well microtiter plate (Costar, Cambridge, Massachusetts, USA), and the plate was incubated overnight at 4℃. After washing, each well was reacted with serum samples that were diluted 1:100 with 0.05% Tween 20. After incubation at 37℃ for 1 hr, a 1:10,000 dilution of horseradish peroxidase-conjugated goat anti-human IgG (Bethyl Laboratories, Montgomery, Texas, USA) was applied, and the plate was incubated at 37℃ for 1 hr. After several washes, freshly prepared
o-phenylenediamine dihydrochloride (Sigma-Aldrich) was added, and the reaction was stopped by adding 8 N H
2SO
4. The IgG antibody titers were determined at the optical density of 490 nm.
The blood samples (n=1,036) from Jeju-do were examined for the presence of T. gondii B1 gene using PCR. The DNeasy blood and tissue kit (Qiagen, Hilden, Germany) was used for isolation of the genomic DNA of T. gondii. To amplify the 497 bp fragment of the gene, PCR was carried out using the following forward Toxo 497 (5'-AGCAAACAC-CGACGAACTCT-3') and reverse Toxo 497 (5'-CATGGTTTGCATTTTGTGG-3') primers. The smart 2X PCR Pre-mix (Solgent, Daejeon, Korea) was used with the following conditions: 94℃ for 5 min, followed by 35 cycles of 94℃ for 60 sec, 55℃ for 55 sec, and 72℃ for 60 sec. The conventional PCR products were analyzed by 1% agarose gel electrophoresis and stained with ethidium bromide.
Statistical analysis
To analyze the risk factors for toxoplasmosis, the chi-square test was applied. P<0.05 was considered statistically significant.
RESULTS
The serum IgG positive rate for
T. gondii, as analyzed by ELISA, was 8.0% (89 positives among 1,114 sera) in Seoul and 11.3% (117 positives among 1,036 sera) in Jeju-do (
Tables 1,
2). The average seropositive rate was 9.6% among all 2,150 residents (
Table 1). The overall seroprevalence was a little higher in Jeju-do than in Seoul, although this difference was not statistically significant (
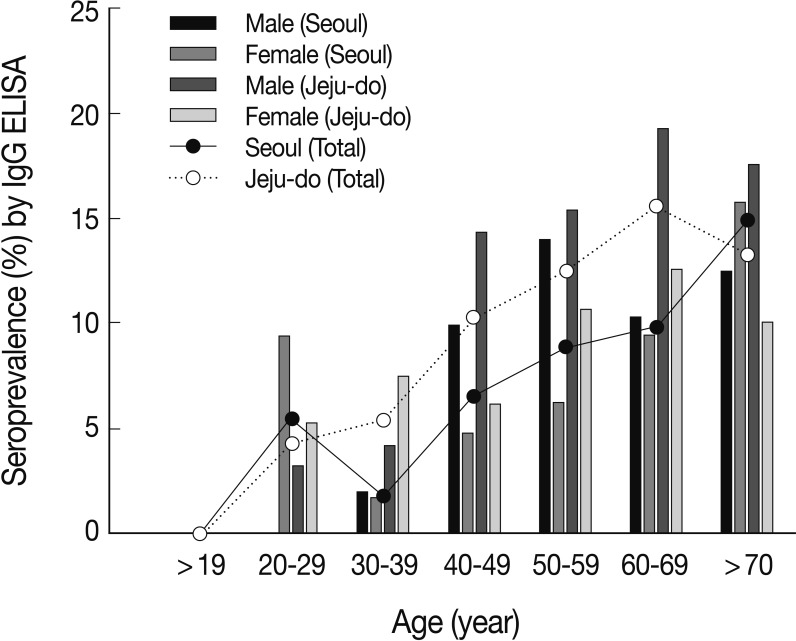
P>0.05). By age group, however, the seroprevalence appeared to be consistently higher in Jeju-do than in Seoul through the age groups of 30-39, 40-49, 50-59, and 60-69 years (
Fig. 1). In both districts, aged residents, particularly, those >40 years of age displayed markedly higher seroprevalences than younger residents (
P<0.05) (
Fig. 1). In Seoul, the highest positive rate, 14.9%, revealed in residents ≥70 years old, whereas in Jeju-do, the highest prevalence, 15.6% (
Fig. 1) was evident in those in their 60s. There were also differences in the seropositive rate of male and female residents. Males usually showed higher seropositive rate than females in Seoul and Jeju-do (
Table 1;
Fig. 1). Particularly in Jeju-do, males showed higher seroprevalence than females with the exception of the age groups 20-29 year old and 30-39 year old age groups (
Fig. 1). Overall, however, the sex difference of the seroprevalence was not statistically significant (
P>0.05) (
Table 1).
The results of the questionnaire study on epidemiologic factors related with
T. gondii infection showed several positive findings, although statistical significance was not confirmed for all of the positive factors (
Tables 2,
3). With regard to occupation, the 18.2% seropositive rate among Jeju-do residents who engaged in agriculture was markedly higher than the average value of 11.3%, although there was no statistical significance (
P>0.05) (
Table 2). Similarly, officers and housewives in Seoul and Jeju-do exhibited slightly lower seroprevalences (5.8-6.6% and 3.9-6.3%, respectively) than the average values (8.0% and 11.3%, respectively). Again, there was no statistical significance also (
P>0.05) (
Table 2).
The residents who preferred to eat a vegetarian diet were less likely to have infection with
T. gondii (
Table 3). The role of this factor was statistically significant particularly in Seoul (
P<0.05). Jeju-do residents who drank bottled water were significantly less likely to get infections (
P<0.05) (
Table 3). Other factors, including the history of contact with animals and travel abroad, did not appear to be related with
T. gondii infection both in Seoul and Jeju-do (
Table 3).
The B1 gene of T. gondii was negative in all of the 1,036 blood samples collected from Jeju-do (samples from Seoul were not examined for the B1 gene), whereas the positive control containing T. gondii RH tachyzoites exhibited positive reaction band in PCR (data not shown).
DISCUSSION
The latex agglutination test (LAT) has been one of the most reliable diagnostic methods for toxoplasmosis for almost 4 decades [
7,
8,
20]. However, its sensitivity has been estimated to be lower than that by ELISA both for serum and cerebrospinal fluid [
11]. Therefore, nowadays in Korea, ELISA is more popularly used than LAT to estimate the seroprevalence of toxoplasmosis [
12-
19,
21-
24]. ELISA can accurately measure IgG, IgM, IgA, or IgE antibodies [
25]. Detection of IgG antibody implies a chronic latent infection, whereas detection of IgM or IgA antibody is indicative of an acute infection [
21,
25]. However, IgM ELISA has a risk of false-positive results due to anti-nuclear antibodies or rheumatoid factor, or of detection of residual or persistent IgM months or even years after the primary infection [
25]. Alternatively, IgG avidity test is performed to detect acute cases [
25-
27], and PCR for the
T. gondii B1 gene is done to detect congenital or chronic clinical cases [
28,
29].
In the present study, IgG ELISA and PCR for the T. gondii B1 gene were carried out. All of the PCR-tested blood samples from Jeju-do revealed negative results. This may indicate that there were no acute clinical toxoplasmosis cases among the subjects examined. Unless a subject is suffering from acute infection, it is less likely for the T. gondii B1 gene to be detected from blood. Meanwhile, in IgG ELISA, 8.0% of residents in Seoul and 11.3% in Jeju-do revealed positive results. The IgG positive rates were higher in males than in females, and those from the forties to the seventies were more likely to be infected than younger individuals.
In the questionnaire, residents who preferred to eat a vegetarian diet and to drink bottled water were revealed to have a significantly lower (P<0.05) seroprevalence than those who ate meat and who consumed groundwater or well water. Those engaged in agriculture had a higher rate of seropositivity, whereas office workers and housewives tended to show lower seroprevalence, although there was no statistical significance (P<0.05) related with these occupation factors. It seems highly plausible that meat consumption is more closely related to infection with T. gondii than other possible factors in these 2 districts of Korea. Similarly, the higher seropositive rate in Jeju-do than in Seoul seems to be related to eating habits. It should be ruled out that the significantly lower seropositive rate among those who drank bottled water than those who consumed grounwater or well water might have been due to a lower risk of infection with T. gondii oocysts through bottled water.
Compared with previous studies conducted in various localities from 1960 until 2009, the results of the present study demonstrated fairly high seroprevalence of
T. gondii infection among residents of Seoul and Jeju-do (
Table 4;
Fig. 2). For example, in Seoul, 1.1-7.0% seroprevalence was reported in 1982-1992 [
7-
11]. Thereafter, among children under 10 years of age in Seoul, a 1997 study revealed 7.7% seropositivity [
13]. However, pregnant women in Seoul showed a prevalence of only 0.9% in 2005 [
18]. Therefore, the prevalence of 8.0% in the present study is the highest seroprevalence of toxoplamosis ever reported from Seoul. With regard to Jeju-do, the seroprevalence was first studied in 1989 and 5.8% seroprevalence was reported from patients in a hospital [
10]. Since then, several studies have reported the seroprevalence of toxoplasmosis in Jeju-do. A survey of high school students and adult hospital patients in Jeju-do revealed 5.5% and 12.9% seroprevalence, respectively [
14]. In 2011 examination of outpatients of a general hospital in Jeju-do revealed a 13.2% IgG ELISA positive rate [
22]. Compared with these reported seroprevalences, the 11.3% seroprevalence observed in the present study appears to indicate a sustanied, rather than decreased, level in Jeju-do.
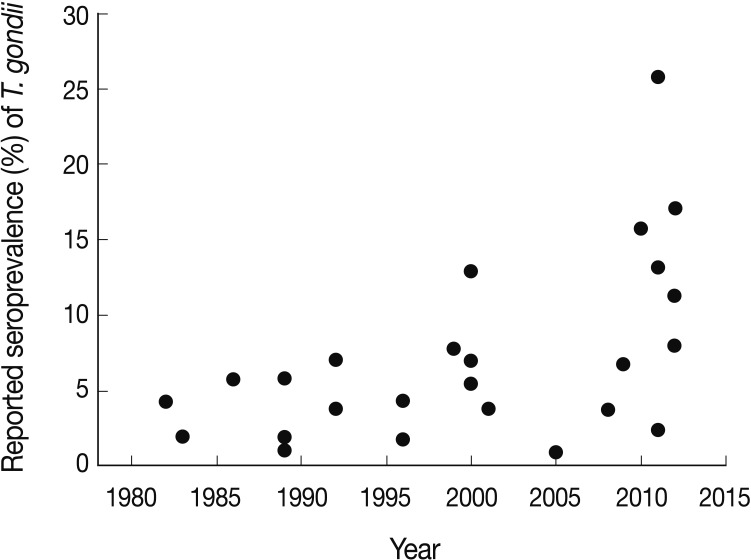
In recent years, an increasing tendency in the seroprevalence of toxoplasmosis in Korea is evidently recognizable (
Table 4;
Fig. 2). Particularly, on islands in Gangwha-gun, the seroprevalence among residents were 15.8% in 2010 and 25.8% in 2011 which was the highest figure ever reported [
23]. Subsequently, in Cheorwon-gun, the IgG ELISA seropositive rate was also high, at 17.0% [
24]. The reason for this increasing tendency of seroprevalence is unclear, although an increase in the number of stray cats [
30] and more popular consumption of meat, including pork, by Koreans [
31] can be suggested as the possible reasons. Nevertheless, it should also be ruled out that the serologic techniques to detect IgG antibodies have been much improved and became more sensitive compared to those used in previous studies. This issue should be clarified in the near future.
The results of the present study strongly suggest that public health attention should be paid to toxoplasmosis prevalence in Korea.
ACKNOWLEDGMENTS
This study was supported by a research grant from The Korea National Institute of Health, Ministry of Health and Welfare, the Republic of Korea (no. 800-20110036). We would like to thank staff of The Korea Association of Health Promotion for providing the sera and blood samples for this study. We have no special conflict of interest related with this study.
References
- 1. Cenci-Goga BT, Rossitto PV, Sechi P, McCrindle CME, Cullor JS. Toxoplasma in animals, food, and humans: An old parasite of new concern. Foodborne Pathog Dis 2011;8:751-762.
- 2. Weiss LM, Dubey JP. Toxoplasmosis: A history of clinical observations. Int J Parasitol 2009;39:895-910.
- 3. Tenter AM, Heckeroth AR, Weiss LM. Toxoplama gondii: from animal to humans. Int J Parasitol 2000;30:1217-1258.
- 4. Montoya JG, Remington JS. Management of Toxoplasma gondii infection during pregnancy. Clin Infect Dis 2008;47:554-566.
- 5. Dubey JP, Jones JL. Toxoplasma gondii infection in humans and animals in the United States. Int J Parasitol 2008;38:1257-1278.
- 6. Soh CT, Lee SJ, Ahn YG. Latent infection by Toxoplasma gondii in Korea. Yonsei Med J 1960;1:52-54.
- 7. Choi WY, Yoo JE, Kim WG. Toxoplasma antibodies by indirect latex agglutination tests in St. Mary's Hospital patients. Korean J Parasitol 1982;20:33-37. (in Korean).
- 8. Choi WY, Yoo JE, Chung CS, Paik KK, Cho SN. Toxoplasma antibodies by indirect latex agglutination tests in National Seoul Mental Hospital patients. Korean J Parasitol 1983;21:281-285. (in Korean).
- 9. Yoo JA, Choi PH. The prevalence of antibodies for Toxoplasma in children. New Med J 1986;29:1644-1648. (in Korean).
- 10. Choi WY, Nam HW, Youn JH, Kim WS, Kim WG. Toxoplasma antibody titers by indirect latex agglutination test in Kangnam St. Mary's Hospital and Cheju Medical Center. Korean J Parasitol 1989;27:171-175.
- 11. Choi WY, Nam HW, Youn JH, Kim DJ, Kong Y, Kang SY, Cho SY. Detection of antibodies in serum and cerebrospinal fluid to Toxoplasma gondii by indirect latex agglutination test and enzyme-linked immunosorbent assay. Korean J Parasitol 1992;30:83-90.
- 12. Ryu JS, Min DY, Ahn MH, Choi HG, Rho SC, Shin YJ, Choi B, Joo HD. Toxoplasma antibody titers by ELISA and indirect latex agglutination test in pregnant women. Korean J Parasitol 1996;34:233-238.
- 13. Kook J, Lee HJ, Kim BI, Yun CK, Guk SM, Seo M, Park YK, Hong ST, Chai JY. Toxoplasma gondii antibody titers in sera of children admitted to the Seoul National University Hospital. Korean J Parasitol 1999;37:27-32.
- 14. Yang HJ, Jin KN, Park YK, Hong SC, Bae JM, Lee SH, Choi HS, Hwang HS, Chung YB, Lee NS, Nam HW. Seroprevalence of toxoplasmosis in the residents of Cheju island, Korea. Korean J Parasitol 2000;38:91-93.
- 15. Hong SC, Yang HJ, Bae JM, Choi HS, Hwang HS, Oh HK, Yun DH. Seroprevalence and risk factors of Toxoplasma gondii infection in high school students in Cheju Province. Korean J Prev Med 2000;33:271-279. (in Korean).
- 16. Lee YH, Noh HJ, Hwang OS, Lee SK, Shin DW. Seroepidemiological study of Toxoplasma gondii infection in the rural area Okcheon-gun, Korea. Korean J Parasitol 2000;38:251-256.
- 17. Bae JM, Yang HJ, Hong SC. The seroprevalence of Toxoplasma gondii infection in teachers of child-bearing age in Cheju Island. Korean J Prev Med 2001;34:444-446. (in Korean).
- 18. Song KJ, Shin JC, Shin HJ, Nam HW. Seroprevalence of toxoplasmosis in Korean pregnant women. Korean J Parasitol 2005;43:69-71.
- 19. Han K, Shin DW, Lee TY, Lee YH. Seroprevalence of Toxoplasma gondii infection and risk factors associated with seropositivity of pregnant women in Korea. J Parasitol 2008;94:963-965.
- 20. Shin DW, Cha DY, Hua QJ, Cha GH, Lee YH. Seroprevalence of Toxoplasma gondii infection and characteristics of seropositive patients in general hospitals in Daejeon, Korea. Korean J Parasitol 2009;47:125-130.
- 21. Ko YH, Lee M, Shin SY, Koo SH, Song JH, Kim J, Kwon KC. Seroprevalence of toxoplasmosis in pregnant women in Daejeon, Korea. Lab Med Online 2011;1:190-194. (in Korean).
- 22. Hong SJ, Chong CK, Lee K, Kim TS, Hong YP, Ahn HJ, Kim HY, Ko AR, Kim YJ, Nam HW. Maintained seroprevalence of toxoplasmosis among the residents of Jeju island, Korea. Korean J Parasitol 2011;49:309-311.
- 23. Yang Z, Cho PY, Ahn SK, Ahn HJ, Kim TS, Chong CK, Hong SJ, Cha SH, Nam HW. A surge in the seroprevalence of toxoplasmosis among the residents of island in Gangwha-gun, Incheon, Korea. Korean J Parasitol 2012;50:191-197.
- 24. Ahn HJ, Cho PY, Ahn SK, Kim TS, Chong CK, Hong SJ, Cha SH, Nam HW. Seroprevalence of toxoplasmosis in the residents of Cheorwon-gun, Gangwon-do, Korea. Korean J Parasitol 2012;50:225-227.
- 25. Candolfi E, Pastor R, Huber R, Filisetti D, Villard O. IgG avidity assay firms up the diagnosis of acute toxoplasmosis on the first serum sample in immunocompetent pregnant women. Diagn Microbiol Infect Dis 2007;58:83-88.
- 26. Leite M, Siciliano S, Rocha LS, Justa MT, César KR, Granato CF. Correlation between specific IgM levels and percentage IgG-class antibody avidity to Toxoplasma gondii. Rev Inst Med Trop Sao Paulo 2008;50:237-242.
- 27. Gay-Andrieu F, Fricker-Hidalgo H, Sickinger E, Espern A, Brennier-Pinchart MP, Braun HB, Pelloux H. Comparative evaluation of the ARCHITECT Toxo IgG, IgM and IgG Avidity assays for anti-Toxoplasma antibodies detection in pregnant women sera. Diagn Microbiol Infect Dis 2009;65:279-287.
- 28. Lee JA, Kim DH, Kim YK, Chung EH, Choi JH, Lee HJ, Chi JG, Chai JY, Lee YH. Two cases of congenital toxoplasmosis diagnosed by polymerase chain reaction. Infect Chemother 2003;35:45-52. (in Korean).
- 29. Lee SE, Hong SH, Lee SH, Jeong YI, Lim SJ, Kwon OW, Kim SH, You YS, Cho SH, Lee WJ. Detection of ocular Toxoplasma gondii infection in chronic irregular recurrent uveitis by PCR. Korean J Parasitol 2012;50:229-231.
- 30. Lee SE, Kim JY, Kim YA, Cho SH, Ahn HJ, Woo HM, Lee WJ, Nam HW. Prevalence of Toxoplasma gondii infection in stray and household cats in regions of Seoul, Korea. Korean J Parasitol 2010;48:267-270.
- 31. Choi WY, Nam HW, Kwak NH. Foodborne outbreaks of human toxoplasmosis. J Infect Dis 1997;175:1280-1282.
Fig. 1Age- and sex-specific seroprevalence of toxoplasmosis among residents in Seoul and Jeju-do assayed by IgG ELISA. The seroprevalence was generally higher in Jeju-do than in Seoul and in males than in females both in Seoul and Jeju-do, although these differences were not statistically significant (P>0.05).
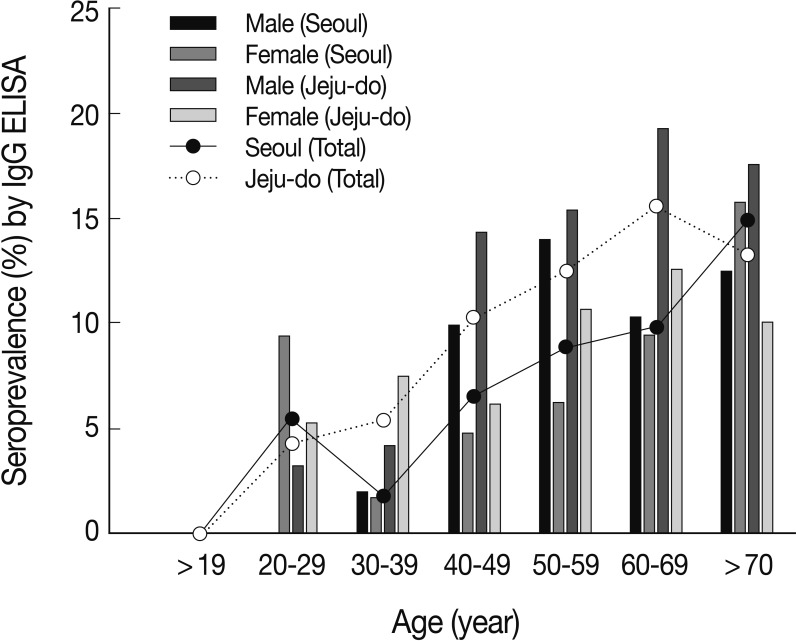
Fig. 2Chronologic view of the seroprevalence of toxoplasmosis reported in Korea (1982-2012) based on data in
Table 4 [
7-
24]. Each point represents % seropositive rate for each subjected group surveyed. Note that the seroprevalence in recent years (2010-2012) showed an increasing tendency.

Table 1.Seroprevalence
a of
Toxoplasma gondii infection among residents in Seoul and Jeju-do
Table 1.
|
District |
Male
|
Female
|
Total
|
|
No. examined |
No. positive (%) |
No. examined |
No. positive (%) |
No. examined |
No. positive (%) |
|
Seoul |
426 |
43 (10.1)b
|
688 |
46 (6.7)b
|
1,114 |
89 (8.0)d
|
|
Jeju-do |
479 |
65 (13.6)c
|
557 |
52 (9.3)c
|
1,036 |
117 (11.3)d
|
|
Total |
905 |
108 (11.9) |
1,245 |
98 (7.9) |
2,150 |
206 (9.6) |
Table 2.Seroprevalence of T. gondii infection according to the occupation of subjects in Seoul and Jeju-do
Table 2.
|
Type of occupation |
Seoul
|
Jeju-do
|
Total
|
|
No. examined |
No. ositive (%) |
No. examined |
No. positive (%) |
No. examined |
No. positive (%) |
|
Agriculture |
7 |
0 (0.0) |
165 |
30 (18.2)a
|
172 |
30 (17.4) |
|
Livestock |
1 |
0 (0.0) |
6 |
0 (0.0) |
7 |
0 (0.0) |
|
Fisheries |
0 |
0 (0.0) |
8 |
1 (12.5) |
8 |
1 (12.5) |
|
Officeb
|
207 |
12 (5.8) |
126 |
8 (6.3) |
333 |
20 (6.0) |
|
Housewifec
|
106 |
7 (6.6) |
76 |
3 (3.9) |
182 |
10 (5.5) |
|
Forestry |
6 |
0 (0.0) |
2 |
1 (50.0) |
8 |
1 (12.5) |
|
Mining |
2 |
1 (50.0) |
2 |
0 (0.0) |
4 |
1 (25.0) |
|
Services |
7 |
1 (7.1) |
35 |
3 (8.6) |
42 |
4 (9.5) |
|
Miscellaneous |
778 |
68 (8.7) |
616 |
71 (11.5) |
1,394 |
139 (10.0) |
|
Total |
1,114 |
89 (8.0) |
1,036 |
117 (11.3) |
2,150 |
206 (9.6) |
Table 3.Relationship of epidemiologic factors and serologic results of T. gondii infection among residents in Seoul and Jeju-do
Table 3.
|
Epidemiologic factor |
Seoul
|
Jeju-do
|
Total
|
|
No. seropositive (Ta) |
No. sero-negative |
No. seropositive (Ta) |
No. sero-negative |
No. seropositive (Ta) |
No. sero-negative |
|
Vegetarian diet |
11b (21) |
255 |
12 (16) |
136 |
23b (40) |
391 |
|
No |
78b (67) |
770 |
105 (100) |
783 |
183b (166) |
1,553 |
|
Using bottled water |
49 (47) |
551 |
44b (56) |
457 |
93 (105) |
1,008 |
|
No |
40 (41) |
474 |
73b (60) |
462 |
113 (101) |
936 |
|
Cooked food intake |
80 (81) |
942 |
83 (87) |
688 |
163 (172) |
1,630 |
|
No |
9 (7) |
83 |
34 (29) |
231 |
43 (34) |
314 |
|
Contact with animals |
15 (12) |
144 |
28 (21) |
166 |
43 (34) |
310 |
|
No |
74 (76) |
881 |
89 (95) |
753 |
163 (172) |
1,634 |
|
History of travel abroad |
24 (28) |
333 |
50 (54) |
430 |
74 (80) |
763 |
|
No |
65 (60) |
692 |
67 (62) |
489 |
132 (126) |
1,181 |
Table 4.Comparison of Toxoplasma gondii seropositive rates in Korea reported by different authors
Table 4.
|
Authors (year) |
Subjects |
Surveyed area |
No. positive/ No. examined |
Seropositive rate (%) |
Assay method |
Reference |
|
Soh et al. (1960) |
Residents |
Korea |
21/373 |
5.8 |
Skin test |
[6] |
|
Choi et al. (1982) |
Patients in a university hospital |
Seoul |
18/421 |
4.3 |
LAa
|
[7] |
|
Choi et al. (1983) |
Mental patients |
Seoul |
11/573 |
1.9 |
LA |
[8] |
|
Yoo and Choe (1986) |
Children ( < 15 years) |
Seoul |
7/120 |
5.8 |
Hemag-glutination |
[9] |
|
Choi et al. (1989) |
Patients in a hospital |
Seoul |
19/1,019 |
1.9 |
LA |
[10] |
|
Asthma patients |
Seoul |
11/1,030 |
1.1 |
LA |
|
|
Patients in a hospital |
Jeju-do |
45/780 |
5.8 |
LA |
|
|
Choi et al. (1992) |
Neurologic patients |
Seoul |
76/2,016 |
3.8 |
LA |
[11] |
|
Neurologic patients |
Seoul |
142/2,016 |
7.0 |
ELISA |
|
|
Ryu et al. (1996) |
Pregnant women |
Gyeonggi-do |
39/899 |
4.3 |
ELISA |
[12] |
|
High school students |
Gyeonggi-do |
4/218 |
1.8 |
ELISA |
|
|
Kook et al. (1999) |
Under 10-year children |
Seoul |
42/542 |
7.7 |
LA |
[13] |
|
Yang et al. (2000) |
Students |
Jeju-do |
250/4,570 |
5.5 |
ELISA |
[14] |
|
Adults |
Jeju-do |
61/474 |
12.9 |
ELISA |
|
|
Hong et al. (2000) |
High school students |
Jeju-do |
250/4,320 |
5.5 |
ELISA |
[15] |
|
Lee et al. (2000) |
Residents |
Okcheon-gun |
74/1,109 |
6.9 |
ELISA |
[16] |
|
Bae et al. (2001) |
Teachers of childbearing age |
Jeju-do |
12/314 |
3.8 |
LA/ELISA |
[17] |
|
Song et al. (2005) |
Pregnant women |
Seoul |
51/5,725 |
0.9 |
ELISA |
[18] |
|
Han et al. (2008) |
Pregnant women |
Daejeon |
13/351 |
3.7 |
ELISA/LA |
[19] |
|
Shin et al. (2009) |
Patients in a university hospital |
Daejeon |
85/1,265 |
6.6 |
LA |
[20] |
|
|
|
84/1,265 |
6.7 |
ELISA |
|
|
Ko et al. (2011) |
Pregnant women |
Daejeon |
19/787 |
2.4 |
ELISA |
[21] |
|
Hong et al. (2011) |
Residents |
Jeju-do |
309/2,348 |
13.2 |
ELISA |
[22] |
|
Yang et al. (2012) |
Residents (2010) |
Gyeonggi-do |
195/1,232 |
15.8 |
ELISA |
[23] |
|
Residents (2011) |
Gyeonggi-do |
335/1,296 |
25.8 |
ELISA |
|
|
Ahn et al. (2012) |
Residents |
Gangwon-do |
282/1,661 |
17.0 |
ELISA |
[24] |
|
Lim et al. (2012)b
|
Residents |
Seoul |
89/1,114 |
8.0 |
ELISA |
- |
|
Residents |
Jeju-do |
117/1,036 |
11.3 |
ELISA |
- |