Abstract
In Vietnam, only few cases of cystic echinococcosis have been reported up to now. We report on the first case of cystic echinococcosis involving the central nervous system reported in Vietnam. Our patient, a 14-year-old child, presented with symptoms of headache and progressive tremor in the right hand that had lasted for 1 month and had worsened in the last days before admission. Following the demonstration of a large space occupying brain cyst by computed tomography, a presumptive diagnosis of a brain tumour was made, that was later overruled. Magnetic resonance imaging, a biopsy and serological analysis allowed for the diagnosis of a giant hydatid brain cyst. The patient underwent surgical removal of the cyst and was treated for 6 months post-surgery with albendazole. On follow-up, the clinical symptoms gradually improved, serology became negative and 1.5 years after the surgical intervention the patient was declared to be cured. This case highlights the importance of considering hydatid disease in differential diagnoses, even in regions where Echinococcus infections are considered rare.
-
Key words: Echinococcus granulosus, hydatidosis, brain, Vietnam
Introduction
Cystic echinococcosis (CE) is a zoonotic disease caused by the metacestode larval stage of
Echinococcus granulosus s.l. [
1]. Dogs are the definitive hosts of
E. granulosus, in which the tapeworm develops in the small intestine. These tapeworms release eggs that are excreted via faeces of the definitive host [
2]. The eggs are infective to intermediate hosts, mainly domestic herbivores and omnivores. Once ingested, the larvae develop into hydatid cysts, which form in various organs. Within these cysts, the parasites undergo asexual multiplication. Dogs become infected by eating cyst-infected offal, perpetuating the life cycle [
3].
Humans can become accidental intermediate hosts following ingesting of parasite eggs in contaminated food or water or after direct contact with infected dogs [
1]. This disease mostly occurs in sheep breeding areas with low economic situation and hygiene such as, Western China, Central Asia, South America, Mediterranean countries, and Eastern Africa [
4,
5]. Out of the 10 known
E. granulosus s.l. strains/genotypes, the
E. granulosus s.s. G1 strain, mainly transmitted between dogs and sheep, accounts for nearly 90% of human infections [
6].
In humans, hydatid cysts are mainly found in the liver and lungs, accounting for over 90% of cases. Cysts can also establish in other organs, including the spleen, kidneys, heart, bones, and the central nervous system [
3,
7]. CE can occur in all age classes, from under 1 year old to 75 years old, of which paediatric patients account for a fairly high rate [
8]. The pathogenesis of CE is the result of functional changes of organs resulting from pressure caused by the growing cysts, as well as from anaphylactic reactions when the cyst wall breaks, releasing their content [
7]. For treatment, the World Health Organization recommends the surgical removal of cysts combined with chemotherapy to avoid recurrence. However, some cases can be treated by anthelmintics only, by ultrasound-guided percutaneous aspiration of cyst fluid followed by instillation and re-aspiration of a scolicidal agent (PAIR [puncture, aspiration, injection, and re-aspiration] technique) or are left untreated [
7,
8].
Although CE is endemic in many parts of the world, it remains rarely reported in Vietnam. To date, only 5 confirmed human cases have been described in literature: 3 cases of pulmonary, 1 case of cardiac CE, and 1 case with concomitant cardiac and hepatic CE [
9-
11]. These reports are notable not only for their rarity but also because all but one could be attributed to
E. ortleppi (G5), commonly referred to as the cattle strain. This strain is infrequently associated with human infection worldwide but seems to be emerging in Asia [
12]. Despite these isolated reports, the true burden of CE in Vietnam is likely underestimated due to limited surveillance, non-specific clinical presentation, and restricted access to diagnostic tools. Moreover, the disease is not notifiable in many areas, and transmission risks—such as close human-animal contact and lack of veterinary inspection—persist in rural settings. These conditions suggest that sporadic cases may be overlooked.
Here we present a case of cerebral CE in a 14-year-old Vietnamese child and the outcome of surgical and anthelmintic treatment.
Case Report
On 22 February 2023 a 14-year-old boy was admitted to the National Paediatric Hospital. Upon clinical examination by the physician, the boy presented with symptoms of dull headache in the back of the neck, right hand tremor, and difficulties in writing that lasted for 1 month. A few days before being admitted to the hospital, the patient suffered from progressively worsening severe headache. He vomited several times a day and had a blurred vision. His medical history was normal. The patient lived in a rural area of Quynh Luu district, Nghe An province, and often played with his grandparents’ dog. He had no travel history.
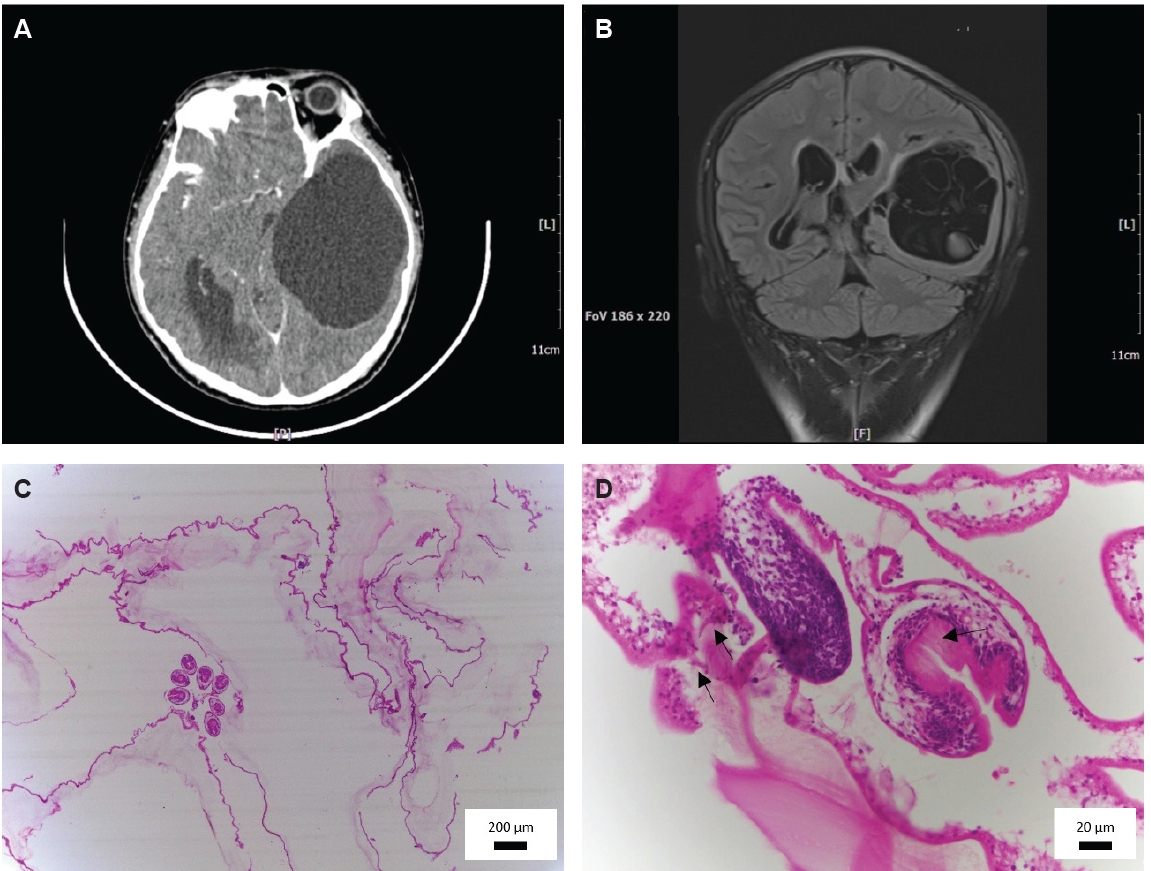
Blood, urine and cerebrospinal fluid samples were obtained, and abdominal ultrasound, chest X-ray and brain computed tomography (CT)-scan were performed on the same day. Hematological and blood biochemical analysis revealed an inflammatory reaction with a high WBC (14,230 cells/mm³) and a neutrophil rate of 81%. Blood and cerebrospinal fluid cultures were negative. Urine tests, abdominal ultrasound, and chest X-ray were normal. A brain CT scan showed a large cyst of 100×71 mm in the left temporo-parietal region compressing the left lateral ventricle and shifting the midline to the right; with dilation of the right lateral ventricle (
Fig. 1A).
The patient was diagnosed with a cystic brain tumour, and it was decided to perform a surgical removal on 27 February 2023. However, during surgery it appeared that the presumed tumour was a large cyst suspected to be caused by a parasite; therefore, no action was taken while waiting for further investigation. Brain magnetic resonance imaging (MRI), performed immediately after the first surgical intervention showed a cystic mass in the left temporal lobe. The cyst was compartmented with membranes dividing the interior into small cysts of different sizes. The cyst fluid was clear and homogeneous, and the cyst was surrounded by a thin wall. The cyst measured 87×64 mm (
Fig. 1B). Serological examination showed a positive result for a commercial
Echinococcus IgG ELISA (Diagnostic Automation/Cortez Diagnostics), with an optical density of 0.532 and a cut-off of 0.3, hinting to the possibility of a brain hydatid cyst.
Based on the presumptive diagnosis, the child underwent a second surgical intervention on 6 March 2023, whereby the cyst was completely excised. The procedure was successful with no rupture of the cyst wall. Intraoperatively, a soft, pinkish-white cyst was identified in the left temporo-occipital region. After removal, the cyst was opened, and it was found to contain multiple smaller cysts, each with a thick and white wall. The cyst fluid appeared transparent, and slightly viscous. A biopsy was subsequently performed to confirm the diagnosis. Histological examination of the biopsy specimen, following hematoxylin and eosin (H&E) staining revealed the presence of
Echinococcus spp. protoscolices (
Fig. 1C,
D).
After surgery, the patient was treated for 2 weeks with ceftriaxone 50 mg/kg twice a day, and with albendazole 15 mg/kg/day divided in 2 doses for 6 months. Ten days after the second operation, the number of WBCs and the rate of neutrophils had become normal (WBCs 9,110 cells/mm³ and neutrophil rate 51.9%). Clinically, the patient no longer suffered from headaches. Moreover, the hand tremors gradually decreased over time, and he could go back to school. The patient was invited for re-examination periodically once a month for 3 months, then every 3 months, to monitor clinical symptoms, blood count and liver enzymes. All test results were normal. On examination on 13 August 2024, all blood test results were normal, and
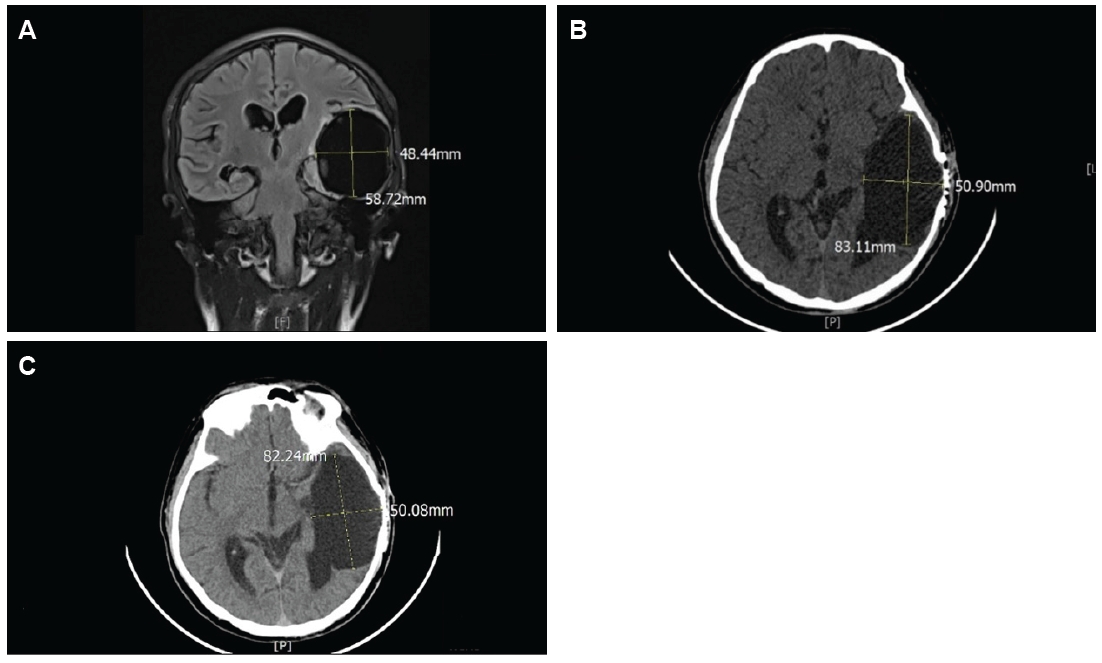
Echinococcus IgG ELISA was negative. The patient was also invited for MRI/CT scans every 6 months to monitor the progression of the postoperative lesion. An MRI performed 8 months post-surgery revealed a cystic structure measuring 59×48 mm, and a CT scan almost 1.5 years post-surgery revealed the same cystic structure (83×51 mm) in the temporal lobe with mild lateral ventricle dilatation (
Fig. 2A,
B). The same structure (82×50 mm) was observed on a CT performed more than 2.5 years post-surgery (
Fig. 2C). At that time the symptoms of headache and hand tremors had completely disappeared, but the memory and learning ability of the boy had declined.
The reporting of the case was approved by National Institute of Malariology, Parasitology and Entomology, Vietnam (No 661/QD-VSR). A consent to participate in the study is not applicable to this case report. Written informed consent was obtained from the patient’s parents for the publication of this case report and accompanying images.
Discussion
This case represents an exceptional presentation of cerebral CE in a child in Vietnam, a country where
E. granulosus infections are very rare. Notably, the 5 previously described CE cases in Vietnam, involved 3 pulmonary cases, 1 cardiac case, and 1 case with concomitant cardiac and hepatic cysts [
9-
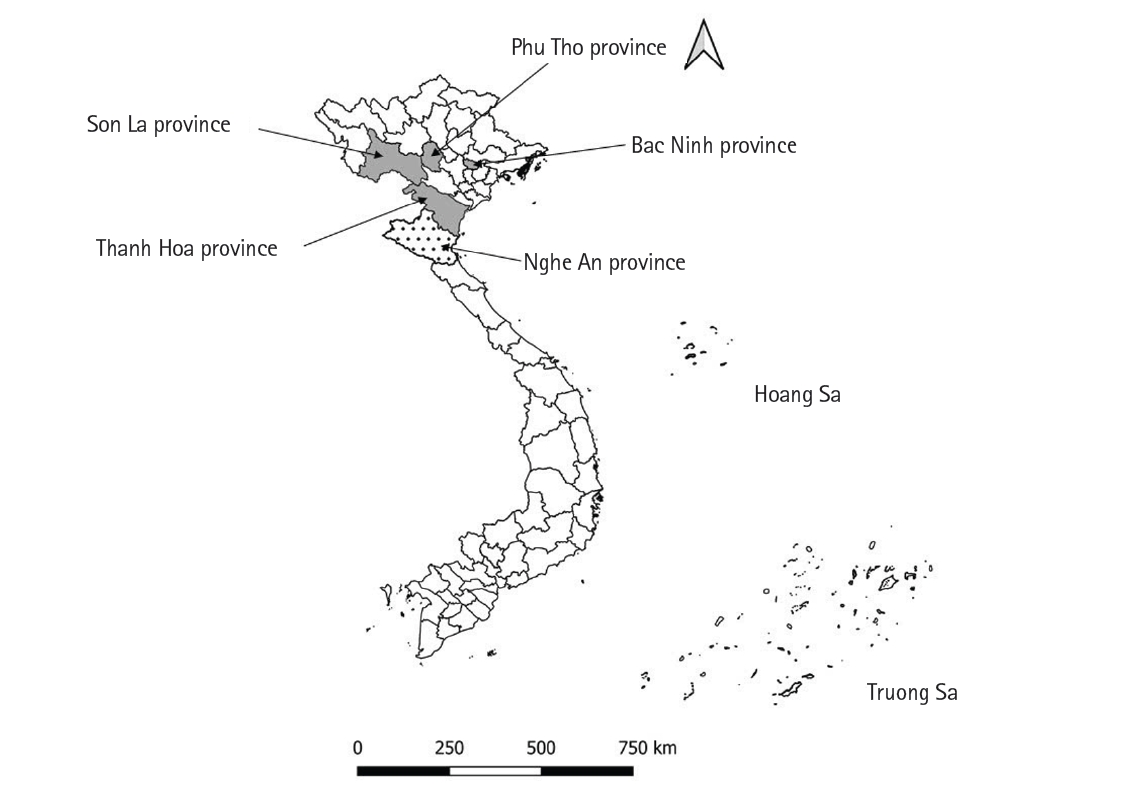
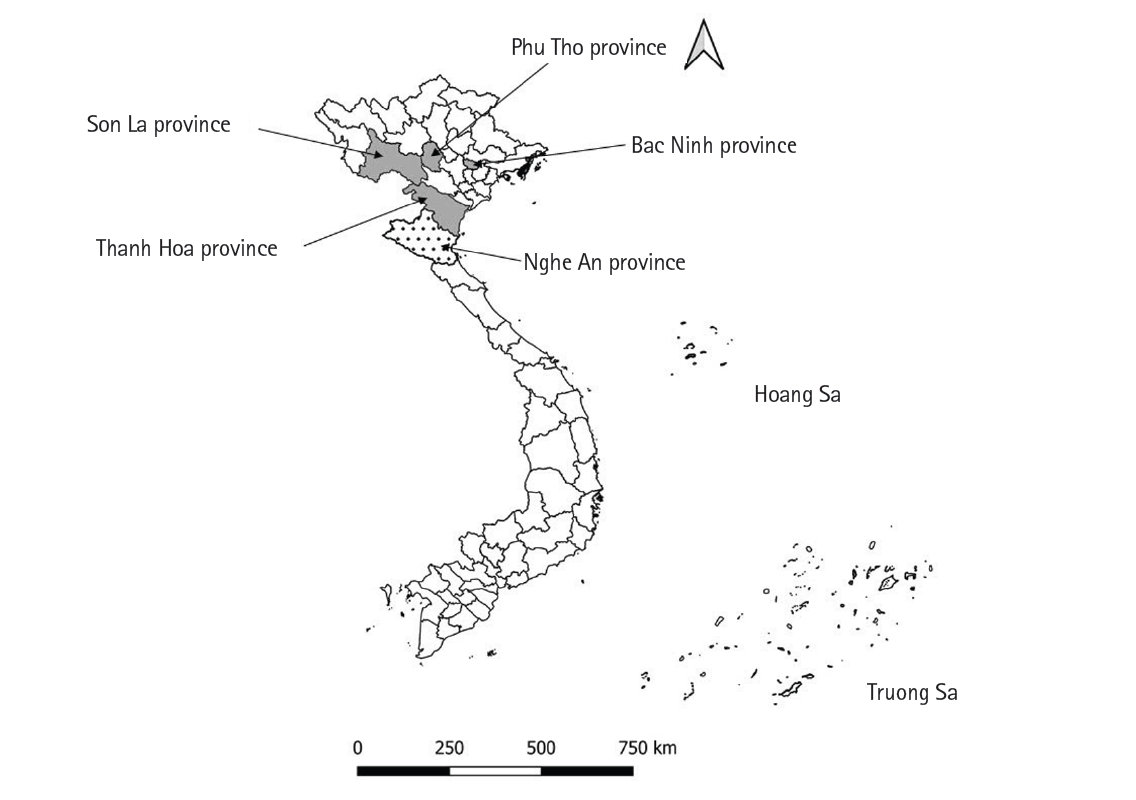
11]. The distribution of these cases (where described in the papers) and our case is shown in
Fig. 3. All but one of the earlier cases were attributed to
E. ortleppi [
9,
10], a genotype uncommonly associated with human infections: a recent review retrieved 19 cases only globally [
12]. Its recent emergence in Asia has been highlighted, yet much remains unknown about its presence in Vietnam. Unfortunately, for our case report, molecular identification of the causative species was not possible, as obtaining the paraffin block of the biopsy for genetic analysis required a formal, multi-step hospital process that was not feasible within the limited timeframe of the patient's follow-up visit.
The transmission dynamics of
Echinococcus in Vietnam are poorly understood. Archaeological data from a 7th-millennium BP forager community suggest that
E. granulosus may have circulated in prehistoric Vietnamese communities, who might have been accidentally exposed through contaminated water sources, shared by wild canids and ruminants (e.g., wild buffalo, deer) [
13]; however, more recent data on animal involvement are scarce. The only documented infection of a final host dates back to 1967, involving a domestic dog [
14], and remarkably, no reports exist of CE in livestock. More recently,
E. ortleppi was also discovered in multiple langur species in Vietnam (
Trachypithecus hatinhensis,
T. delacouri,
Pygathrix nemaeus, and
P. cinerea) [
15,
16], raising the possibility of an underrecognized sylvatic reservoir and transmission route involving wild primates as intermediate hosts.
Cerebral hydatid cysts are extremely rare, occurring in only about 0.4% of human CE cases [
8]. Given this context, and the fact that infections in Vietnam are equally rare, clinical familiarity with cerebral CE is limited. It is therefore unsurprising that the diagnosis was delayed and the lesion was initially mistaken for a brain tumor. Contributing further to this diagnostic challenge was the child’s unusually mild symptomatology despite the presence of a large space-occupying cyst. For a considerable period, the child remained asymptomatic, and only began experiencing subtle neurological signs—such as headaches, right-hand tremors, and writing difficulties—about a month before surgery. These symptoms were non-specific and easily attributed to more common pediatric neurological conditions. In the days preceding surgical intervention, the child developed blurred vision and vomiting, which, although more suggestive of intracranial pressure, still lacked specificity. Cerebral CE was only correctly diagnosed after further imaging, histopathology, and serological testing. As no other cysts were found in this child, a primary cerebral infection is suggested rather than a secondary spread from other organs.
Following World Health Organization guidelines, the patient underwent surgery to remove the cyst, followed by a 6-month course of albendazole (15 mg/kg/day). Throughout treatment, blood tests, liver function, and enzyme levels remained stable, and serological tests eventually turned negative. Postoperative MRI and CT scans were conducted every 6 months. While the child’s symptoms had fully resolved a year and a half after surgery, some cognitive difficulties, particularly with learning and memory, persisted. Neuroimaging also continued to show a residual cyst, highlighting the need for long-term monitoring.
Overall, this case highlights the importance of considering hydatid disease in differential diagnoses, even in regions where Echinococcus infections are considered rare. Diagnosing cerebral CE can be particularly challenging, especially when relying on clinical symptoms and basic neuroimaging, as it often mimics a brain tumour. The lack of epidemiological data on Echinococcus in Vietnam underscores the need for further research. Studies in domestic dogs, livestock, and wildlife are essential to understand the parasite’s transmission, its intermediate hosts, and the genotypes circulating in the region. Given the presence of free-roaming dogs in rural communities, regular deworming programs could be an effective strategy to reduce the risk of human infections. This case serves as a reminder that even rare diseases can appear in unexpected places—and when they do, they can challenge both diagnosis and treatment. Continued surveillance and research will be crucial to uncovering the true burden of echinococcosis in Vietnam and beyond.
Notes
-
Author contributions
Conceptualization: Huong TTT, Lam NV, Trung VT, Binh VTL, Dermauw V, Dorny P. Data curation: Huong TTT, Lam NV, Trung VT. Investigation: Huong TTT, Lam NV, Trung VT. Methodology: Huong TTT, Lam NV, Trung VT. Project administration: Huong TTT. Resources: Huong TTT, Lam NV, Trung VT. Supervision: Huong TTT, Lam NV. Validation: Huong TTT, Lam NV, Trung VT. Visualization: Trung VT. Writing – original draft: Binh VTL, Dermauw V, Dorny P. Writing – review & editing: Binh VTL, Dermauw V, Dorny P.
-
Conflict of interest
The authors have no conflicts of interest to declare.
-
Acknowledgments
We thank the patient’s parents for consenting to provide their son’s medical information. We are grateful to National Paediatric Hospital Vietnam for treatment and closely following up the patient.
Fig. 1.Imaging results of the case. (A) Computed tomography scan prior to first surgery showing a giant cyst (100×71 mm), mimicking a brain tumour. (B) Magnetic resonance imaging image prior to second surgery revealing a giant cyst (87×64 mm) filled with cyst fluid, delineated by a thin wall, and containing membrane structures dividing it in different compartments. (C) Histological image (hematoxylin-eosin staining) of a biopsy of a membrane-like mass obtained after second surgery, showing the cyst wall and Echinococcus spp. protoscolices (100× magnification). (D) Histological image (hematoxylin-eosin staining) of a biopsy of a membrane-like mass obtained after second surgery, showing a Echinococcus spp. protoscolex with hooks (arrows) (400× magnification).
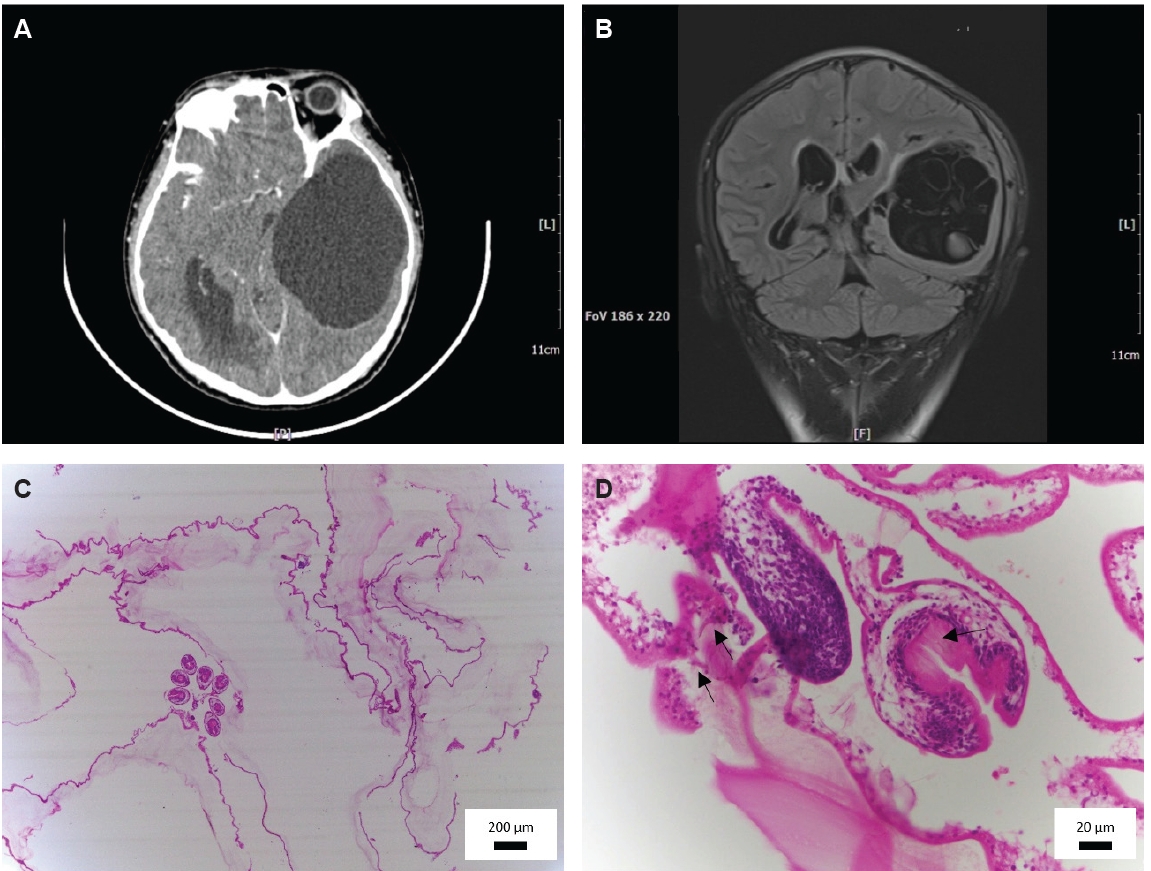
Fig. 2.Follow-up imaging of the case. (A) Magnetic resonance imaging image 8 months after the second surgery revealed a cystic structure measuring 59×48 mm. (B) Computed tomography image 1.5 years after the second surgery revealed 83×51 mm cystic structure in the temporal lobe with mild lateral ventricular dilatation. (C) Computed tomography image 2 years and 8 months after the second surgery revealed 82×50 mm cystic structure in the temporal lobe with mild lateral ventricular dilatation
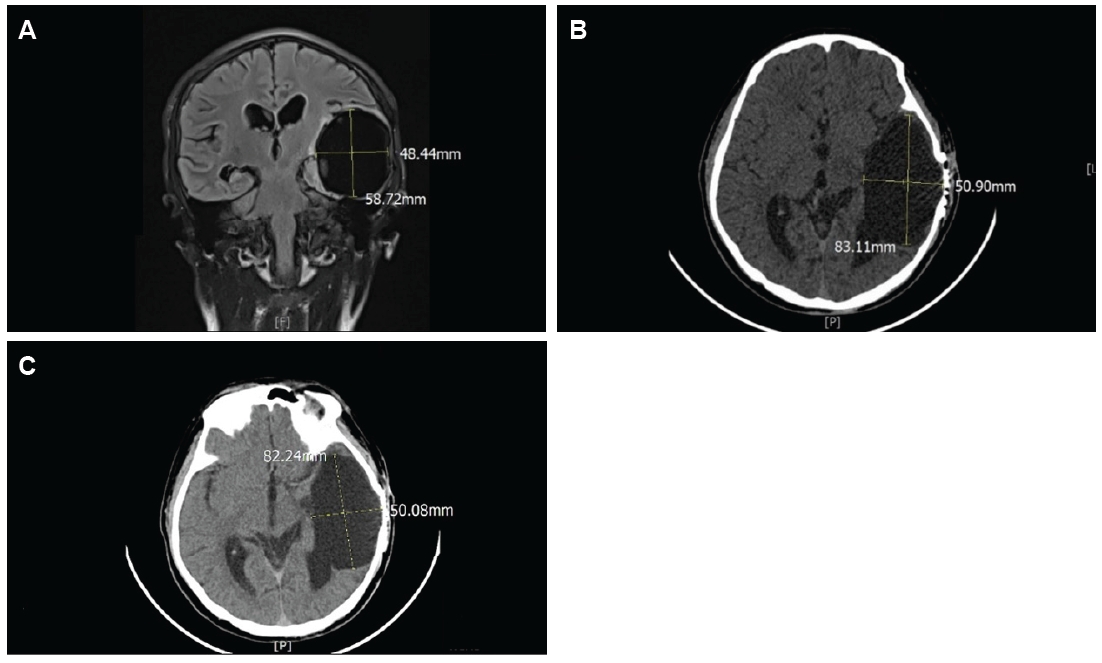
Fig. 3.Distribution of earlier cases and the current case of hydatidosis in Vietnam. Grey indicates provinces with earlier reported cases and the dotted white area denotes the province of origin of our case.
References
- 1. World Health Organization. Echinococcosis [Internet]. 2021 [cited 2025 Nov 25]. Available from: https://www.who.int/news-room/fact-sheets/detail/echinococcosis
- 2. Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev 2004;17:107-35. https://doi.org/10.1128/CMR.17.1.107-135.2004
- 3. Moro P, Schantz PM. Echinococcosis: a review. Int J Infect Dis 2009;13:125-33. https://doi.org/10.1016/j.ijid.2008.03.037
- 4. Wen H, Vuitton L, Tuxun T, et al. Echinococcosis: advances in the 21st century. Clin Microbiol Rev 2019;32:e00075-18. https://doi.org/10.1128/CMR.00075-18
- 5. Hogea M, Ciomaga BF, Muntean A, et al. Cystic echinococcosis in the early 2020s: a review. Trop Med Infect Dis 2024;9:36. https://doi.org/10.3390/tropicalmed9020036
- 6. Alvarez Rojas CA, Romig T, Lightowlers MW. Echinococcus granulosus sensu lato genotypes infecting humans: review of current knowledge. Int J Parasitol 2014;44:9-18. https://doi.org/10.1016/j.ijpara.2013.08.008
- 7. Brunetti E, Kern P, Vuitton DA; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop 2010;114:1-16. https://doi.org/10.1016/j.actatropica.2009.11.001
- 8. Pawlowski Z, Eckert J, Vuitton DA, et al. Echinococcosis in humans: clinical aspects, diagnosis and treatment. In: World Organisation for Animal Health. WHO/OIE manual on echinococcosis in humans and animals: a public health problem of global concern. World Organisation for Animal Health; 2002. p. 20-66.
- 9. Van De N, Le Van D. The first report of two cases of cystic echinococcosis in the lung by Echinococcus ortleppi infection, in Vietnam. Res Rep Trop Med 2017;8:45-51. https://doi.org/10.2147/RRTM.S122014
- 10. De NV, Minh PN, Duyet LV, et al. Two human cases of Echinococcus ortleppi infection in the lung and heart in Vietnam. Korean J Parasitol 2020;58:451-6. https://doi.org/10.3347/kjp.2020.58.4.451
- 11. Nguyen HTT, Pham VT, Duong HD, et al. Concomitant intramyocardial and hepatic hydatid cysts diagnosed by multi-modality imaging: a rare case report. Front Cardiovasc Med 2022;9:1055000. https://doi.org/10.3389/fcvm.2022.1055000
- 12. Yoshida A, Irie T, Le LA, Bui KL, Nawa Y. Echinococcus ortleppi infection in humans: an emerging zoonosis in Asia. Parasitol Int 2024;103:102949. https://doi.org/10.1016/j.parint.2024.102949
- 13. Vlok M, Buckley HR, Domett K, et al. Hydatid disease (Echinococcosis granulosis) diagnosis from skeletal osteolytic lesions in an early seventh-millennium BP forager community from preagricultural northern Vietnam. Am J Biol Anthropol 2022;177:100-15. https://doi.org/10.1002/ajpa.24435
- 14. Le-Van-Hoa , Vu-Ngoc-Tan . Concerning the presence of cestodes, Echinococcus granulosus (Batsch, 1786), in a wild dog, Cyon primaerus (Hodgs) in South Vietnam. Bull Soc Pathol Exot Filiales 1967;60:64-71.
- 15. Plesker R, Nadler T, Dinkel A, Romig T. A case of an Echinococcus ortleppi infestation in a red-shanked douc langur (Pygathrix nemaeus) in northern Vietnam. Vietnam J Primatol 2009;3:75-81.
- 16. Thanh VD, Nam VH, Anh LTL, et al. Transmission of Echinococcus ortleppi at the Endangered Primate Rescue Center, Cuc Phuong National Park. Vietnam J Primatol 2020;3:53-8.

 , Vu Thi Lam Binh2
, Vu Thi Lam Binh2