Abstract
To improve our understanding of the migration of sparganum in humans, we report a case of ocular sparganosis having the migratory episode from the muscle cone to the subconjunctiva. A 34-year-old woman was admitted to the Hospital of Anhui Medical University (Hefei, China), in December 2019. She presented with conjunctival hemorrhage and recurrent pain in the left eye. A foreign body was found in the muscle cone of the eye. Two months later, a ribbon-like white material was found under the conjunctiva on slit-lamp examination. A long and slender, actively moving parasite was extracted by surgery. The extracted worm was approximately 8 cm long and 2 mm wide. The worm was whitish, wrinkled, ribbon shaped, and had a slightly enlarged scolex. The worm sample was morphologically identified as a plerocercoid larva (sparganum) of the Spirometra tapeworm. Her conjunctival blood suffusion and eye pain ceased within 1 week after operation. She has been in good health without any symptoms during the 2-year follow-up. A case of ocular sparganosis, in which larval worm migrated from the muscle cone to the subconjunctiva is reported from China.
-
Key words: Spirometra tapeworm, sparganum, ocular infection, surgical removal
INTRODUCTION
Sparganosis is a larval cestodiasis by the infection with the plerocercoids of
Spirometra tapeworm. Humans are accidentally infected with these larval worms as intermediate hosts and rarely definitive hosts [
1]. Humans can become infected in a number of ways, mainly by eating raw and inadequately cooked frog/snake meat or by drinking unfiltered/untreated water that contains procercoid laying cyclops. Sparganum, a plerocercoid larva of
Spirometra spp., has been found worldwide but the majority of cases occur in East Asian countries including China [
1–
3].
This parasite can be found in any part of the body. Ocular infection is relatively high in Southeast Asian countries due to poultice.[
4]. The clinical features of ocular sparganosis include swelling of the eyelid, subconjunctival edema, or intraorbital mass in the soft tissue. The common symptoms are lacrimation, pain, and redness of the eye [
5]. Ocular sparganosis is frequently misdiagnosed because a variety of eye diseases can show similar symptoms. We report an interesting case of ocular sparganosis with an episode of migration of the parasite from the muscle cone to the subconjunctiva that occurred in China.
CASE DESCRIPTION
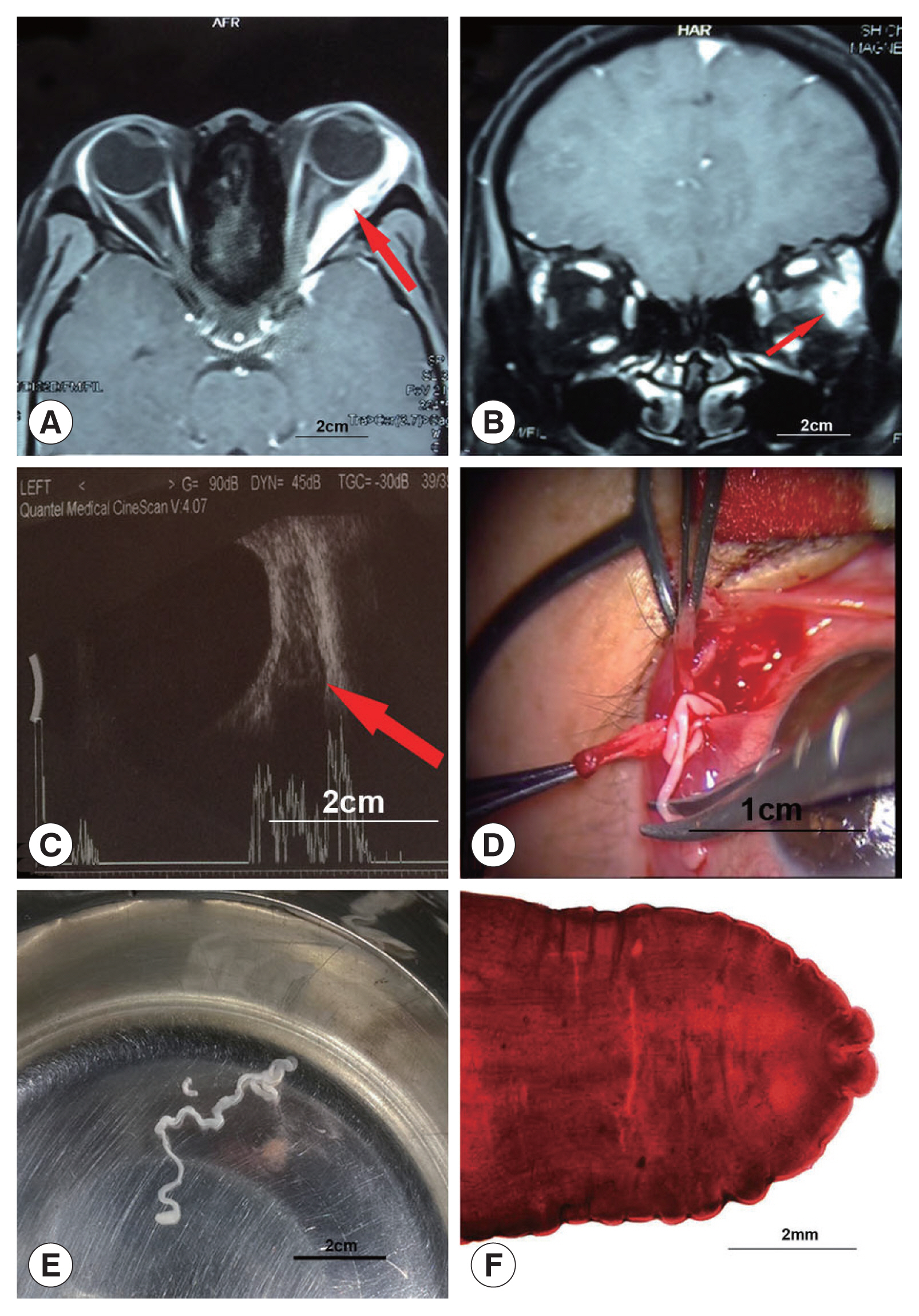
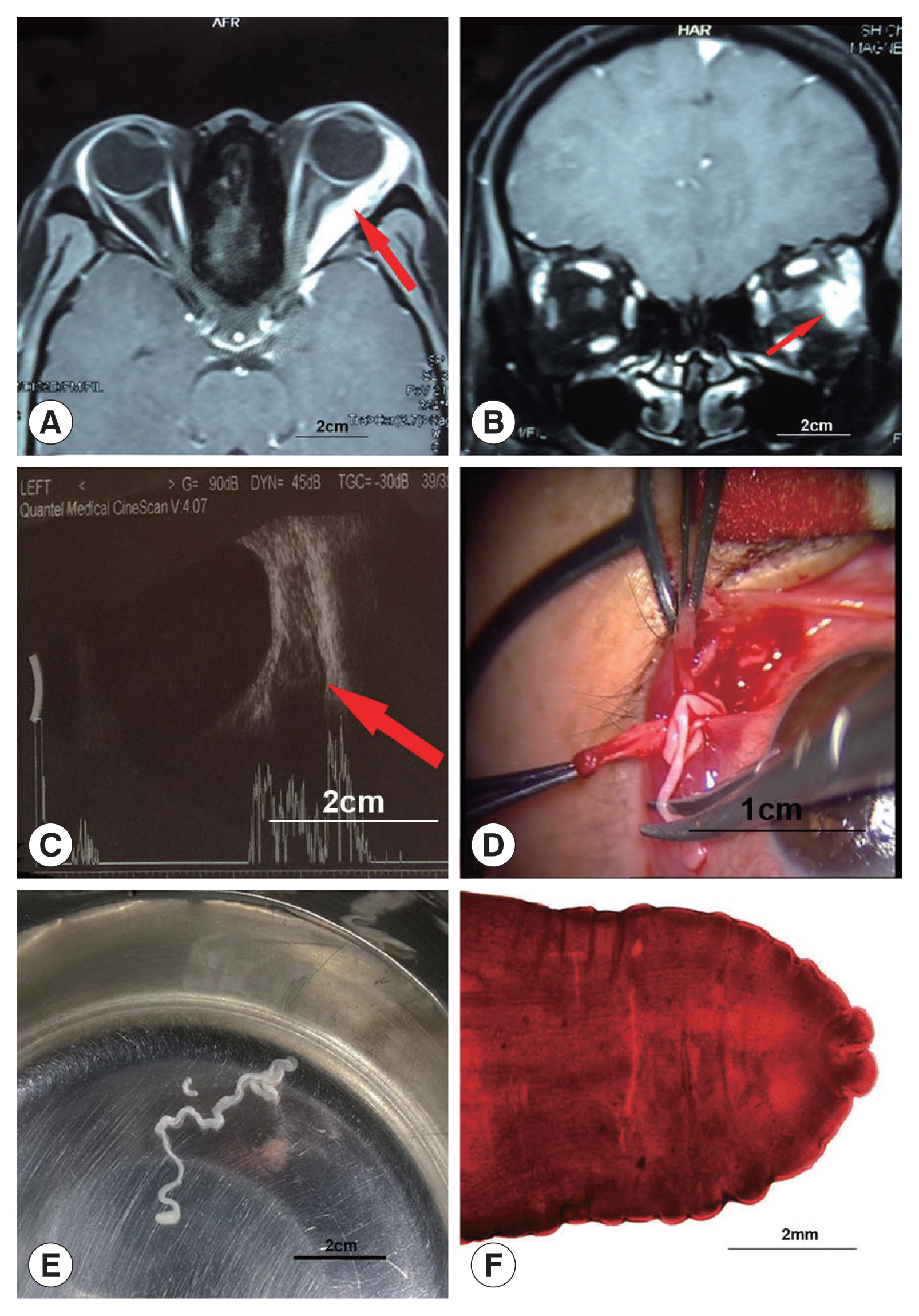
In December 2019, a 34-year-old woman visited our hospital with the complaints of conjunctival blood suffusion and recurrent pain in her left eye. She had no systemic or visual symptoms. She had a history of using pond water to wash her face and eating undercooked frog meat. The patient’s left eyeball was slightly protruding, but ocular motility was normal. The other ophthalmological examinations, including the fundus and visual acuity, were within the normal ranges for both eyes. The thyroid-related indexes, electrocardiogram, radiographic images of the lungs, renal function, and liver function indicated no abnormalities. A magnetic resonance imaging (MRI) scan from another hospital showed a foreign body in the muscle cone close to the lateral rectus in the left eye. On T1-weighted MRI, high signal, extending from the ocular attachment of the lateral rectus muscle to the depth of the orbit, very close to the optic nerve, was detected (
Fig. 1A, B). On ultrasonography of the left eye, abnormal signals and an irregular hypoechoic mass with distinct borders were observed in the posterior part of the eyeball (
Fig. 1C). The patient refused surgery to remove the lesion because of the possibility of damage to vision. As parasitic space-occupying lesions in the orbit are rare, we did not consider a parasitic infection in the initial diagnosis.
Two months later, the patient returned and explained that she experienced a creeping sensation in the left eye. Slit-lamp examination revealed a visible ribbon-like white foreign body under the conjunctiva in the left eye. Surgical exploration recovered a parasite (
Fig. 1D). The extracted worm was approximately 8 cm in length, 2 mm in width, white in color, wrinkled, and ribbon shaped. The worm had a slightly enlarged head (
Fig. 1E). The worm sample was morphologically identified as a plerocercoid larva (sparganum) of
Spirometra tapeworm (
Fig. 1F). Due to improper preservation of the parasites, molecular biological analysis could not be conducted, and the specific identity of the sparganum was not clear. The conjunctival blood suffusion and eye pain ceased 1 week after the operation. At 2-year follow-up, both eyes were examined using computed tomography (CT). No recurrence was found.
DISCUSSION
We report a case of a plerocercoid larva (sparganum) of Spirometra tapeworm infection in the human orbit. In this case, a space-occupying lesion was initially diagnosed and planned for intraorbital surgery. A visible ribbon-like white foreign body under the conjunctiva was found in the left eye with a slit-lamp examination 2 months later. Subconjunctival surgery was performed and the parasitic infection was confirmed. The possibility of parasitic infection should be considered in patients with ocular space-occupying lesions, and the timing of surgery is important.
The diagnosis of the present case was delayed because of the insufficient attention paid to the possibility of ocular parasitic infection. To avoid miss diagnosis of ocular sparganosis, the clinical symptoms of the parasitic infection and findings from related examinations should be confirmed. Human ocular sparganosis manifests with various clinical symptoms, including swelling, redness, and edema of the eyelid or conjunctiva. Our patient presented with conjunctival congestion and subconjunctival yellowish-white granulomatous lesions, which prompted the clinicians to consider the possibility of ocular sparganosis infection. Serological tests and medical imaging examinations are more useful in diagnosing sparganum infection. On ultrasonography, the low echo in the lesion area was irregular, and the orbital mass displayed a linear or columnar shape. Diffuse or nodular masses are typical CT imaging features of orbital sparganosis [
6]. Punctate calcification and diffuse soft tissue infiltration are also commonly observed on CT scans. On MRI, an annular enhanced tunnel is the most characteristic feature of orbital sparganosis. MRI can clearly show the organizational characteristics and location of a space-occupying disease. Elevated eosinophils in routine blood tests can indicate a recent parasitic infection [
7,
8]. Furthermore, enzyme-linked immunosorbent assay can detect anti-sparganosis antibodies in serum with up to 90% sensitivity and specificity. Thus, these measures are highly useful as effective auxiliary diagnostic tools for sparganosis. Worm species can be identified by sequencing [
9–
11]. Unfortunately, due to the improper preservation method of the parasite in this case, further molecular analysis of the parasite could not be carried out. The molecular phylogenetic identification of this sparganum is not clear.
The sparganum can migrate in the human body, invading various tissues and organs. The present case is a report case of sparganum migrating from the cone of the eye to the subconjunctiva. Owing to the postponement of the operation, instead of orbital surgery, which was originally required, ocular surface surgery was performed, which reduced not only the difficulty of the procedure but also the pain of the patient. This case suggests that further study is needed to determine the appropriate timing of surgery for patients with orbital sparganum infection. In patients with orbital infection caused by sparganum, the space for worms to migrate is limited. If the patient shows no deterioration of visual function and no obvious serious complications, the timing of the operation can be determined on the basis of the location of the worm. When the parasite has migrated from the deep to the superficial part of the orbit, surgery may be minimally invasive to the patient. At this stage, the condition of the eye should be closely observed, and the appropriate timing of surgery should be determined.
In conclusion, sparganum has strong mobility and can migrate through the tissues. For the orbit with limited space, it may be a better method to wait until sparganum migrates to the superficial position for surgery. Therefore, it is important to determine the appropriate time for removal of parasites. More case studies are needed to confirm whether surgery can be delayed in patients with orbital infection of sparganosis.
Notes
-
The authors have no conflicts of interest to disclose.
ACKNOWLEDGMENTS
The consent was obtained from the patient for the publication of this case report. This work was supported by a grant from the Foundation of Anhui Medical University (2021xkj 161).
Fig. 1Magnetic resonance imaging (A, B) and ultrasonography (C) show a foreign body in the muscle cone. (D) The sparganum found during the surgical operation of the left eye. (E) The extracted worm is long and slender and actively moving in physiological saline. (F) The anterior portion of the sparganum stained with acetocarmine.
References
- 1. Kim JG, Ahn CS, Sohn WM, Nawa Y, Kong Y. Human sparganosis in Korea. J Korean Med Sci 2018;33:e273. https://doi.org/10.3346/jkms.2018.33.e273
- 2. Ou Q, Li SJ, Cheng XJ. Cerebral sparganosis: a case report. Biosci Trends 2010;4:145-147.
- 3. Liu W, Gong T, Chen S, Liu Q, Zhou H, He J, Wu Y, Li F, Liu Y. Epidemiology, diagnosis, and prevention of sparganosis in Asia. Animals 2022;12:1578. https://doi.org/10.3390/ani12121578
- 4. Anantaphruti MT, Nawa Y, Vanvanitchai Y. Human sparganosis in Thailand: an overview. Acta Trop 2011;118:171-176. https://doi.org/10.1016/j.actatropica.2011.03.011
- 5. Liu Q, Li MW, Wang ZD, Zhao GH, Zhu XQ. Human sparganosis, a neglected food borne zoonosis. Lancet Infect Dis 2015;15:1226-1235. https://doi.org/10.1016/S1473-3099(15)00133-4
- 6. Kubota T, Itoh M. Sparganosis associated with orbital myositis. Jpn J Ophthalmol 2007;51:311-312. https://doi.org/10.1007/s10384-007-0438-1
- 7. Yu MH, Chen CL, Liu XL, Xu XW. Differential diagnosis of a carcinoma of the maxillary sinus that resembles a sparganum infection: a case report. Exp Ther Med 2015;10:1324-1326. https://doi.org/10.3892/etm.2015.2661
- 8. Takeda K, Suzuki J, Nagai H, Watanabe K, Yokoyama A, Ando T, Suzuki J, Ohshima N, Masuda K, Tamura A, Akagawa S, Kitani M, Hebisawa A, Matsui H, Kobayashi N, Maruyama H, Ohta K. Thoracoscopic examination of empyema in a patient with sparganosis mansoni. J Infect Chemother 2016;22:120-123. https://doi.org/10.1016/j.jiac.2015.09.009
- 9. Zhu Y, Ye L, Ding X, Wu J, Chen Y. Cerebral sparganosis presenting with atypical postcontrast magnetic resonance imaging findings: a case report and literature review. BMC Infect Dis 2019;19:748. https://doi.org/10.1186/s12879-019-4396-2
- 10. Jo GD, Lee JY, Hong ST, Kim JH, Han JK. Presumptive case of sparganosis manifesting as a hepatic mass: a case report and literature review. World J Radiol 2016;8:846-850. https://doi.org/10.4329/wjr.v8.i10.846
- 11. Fang L, Wang Y, Gao Q, Yan B, Zhou J. Recurrent eosinophilic pleuritis caused by sparganum infection: A case report and review of the literature. Medicine 2020;99:e20226. https://doi.org/10.1097/MD.0000000000020226
Citations
Citations to this article as recorded by

- Central nervous system sparganosis: An extraordinary case in an adult and a pediatric patient
Yuke Zeng, Xiaoruo Tan, Yuanpeng Hu, Shiquan Lu, Lin Du, Changfeng Xie, Caiwei Zhou, Yingyi Tan, Kewei Fan, Liping Jiang, Wei Liu
International Journal of Infectious Diseases.2026; 168: 108589. CrossRef - Ocular infections in international travelers
Francesca F. Norman, Julio J. González-López, Diego Gayoso-Cantero, Marta Vicente-Antolin, Maria-Dolores Corbacho-Loarte, Rogelio López-Vélez, Marta González-Sanz
Travel Medicine and Infectious Disease.2025; 63: 102789. CrossRef - Hand palm sparganosis: morphologically and genetically confirmed Spirometra erinaceieuropaei in a fourteen-year-old girl, Egypt
Hussein M. Omar, Magdy Fahmy, Mai Abuowarda
Journal of Parasitic Diseases.2023; 47(4): 859. CrossRef - Ocular sparganosis: comment
Amnuay Kleebayoon, Viroj Wiwanitkit
Parasites, Hosts and Diseases.2023; 61(1): 94. CrossRef