Abstract
Sparganosis is one of the common zoonotic diseases caused by infection with the larval plerocercoids (spargana) of the cestode genus Spirometra. While this parasite distributes globally in canine and feline hosts, human infection is predominantly reported in East Asia, especially China, Korea, Japan, and Thailand. Maybe related to the behavior and food culture, this zoonotic disease is rather rare in South Asia to the Middle East. In these areas, sporadic case reports have been appeared mostly in the local medical journals. To draw a solid picture of sparganosis in these non-endemic areas of Asia, we made an extensive literature survey to gather sparganosis cases in the Indian subcontinent and the Middle East.
-
Key words: Spirometra, sparganosis, human, Indian subcontinent, Middle East
Introduction
Sparganosis is one of the well-known zoonotic diseases caused by infection with the larval plerocercoids (sparganum;
pl.=spargana) of cestode of genus
Spirometra, which is a middle-sized tapeworm parasitizing in the small intestine of canine, feline, and other mammalian hosts. This parasite requires 2 intermediate hosts; coracidia hatched from eggs in freshwater are ingested by cyclops (the first intermediate hosts), and develop into procercoids. When procercoids in cyclops are ingested by amphibians (the second intermediate hosts), they grow into plerocercoids (=spargana). Along with the food-chain, reptiles, birds, and mammals including humans can act as the paratenic hosts [
1–
4]. While this parasite distributes globally in canine and feline hosts, human infection is predominantly reported in East and Southeast Asia, especially China [
1], Korea [
2], Japan [
3], and Thailand [
4,
5]. In those highly endemic areas, human infection occurs via 3 ways; 1) as a water-borne disease by ingestion of cyclops contaminated with procercoids, 2) as a food-borne disease by ingestion of uncooked/undercooked meat harboring plerocercoids of second intermediate or paratenic hosts, and 3) direct penetration from contaminated meat used as poultice. Once
Spirometra larvae are ingested by humans, they preferentially migrate into soft subcutaneous tissues to form slowly moving nodular lesions. Although the frequency is far lower than subcutaneous migration, occasionally the larvae migrate into the vital organs such as brain, spinal cord or eyes to cause deleterious results [
1–
4].
In contrast to the high incidence in East and Southeast Asia, this zoonotic disease is rather rare in South Asia to Middle East, maybe related to the behavior and food culture. In those areas, only few sporadic case reports have been appeared mostly in the local medical journals. To draw a solid picture of sparganosis in these non/low-endemic areas in Asia, we made an extensive literature survey to gather sparganosis cases in the Indian subcontinent and Middle East.
Literature survey
We used terms “sparganosis”, “
Spirometra” and the country names like “India”, “Iraq”, and etc. for search. As the first step, we searched published works, mostly case reports, of sparganosis from PubMed (
https://www.ncbi.nlm.nih.gov/pubmed/) in conjunction with Medical Subject Headings (MeSH) in the National Library of Medicine (
https://www.nlm.nih.gov/mesh/). We also searched the related papers using Google Scholar (
https://scholar.google.co.jp/). Then, as the secondary search, we carefully and thoroughly checked the references/citations in each paper.
In India, the first case of human sparganosis was recorded by Datta et al. in Jodhpur in 1982 [
6]. Since then, human sparganosis cases have been reported sporadically from various places of India, 20 cases of which were recently reviewed by Kaur and Shukla [
7] in their case report of cerebral sparganosis. After extensive literature survey, we have found some additional cases which are not included in the list by Kaur and Shukla [
7]. In total, we could gather 25 cases of human sparganosis in India and the results are summarized in
Table 1 [
6–
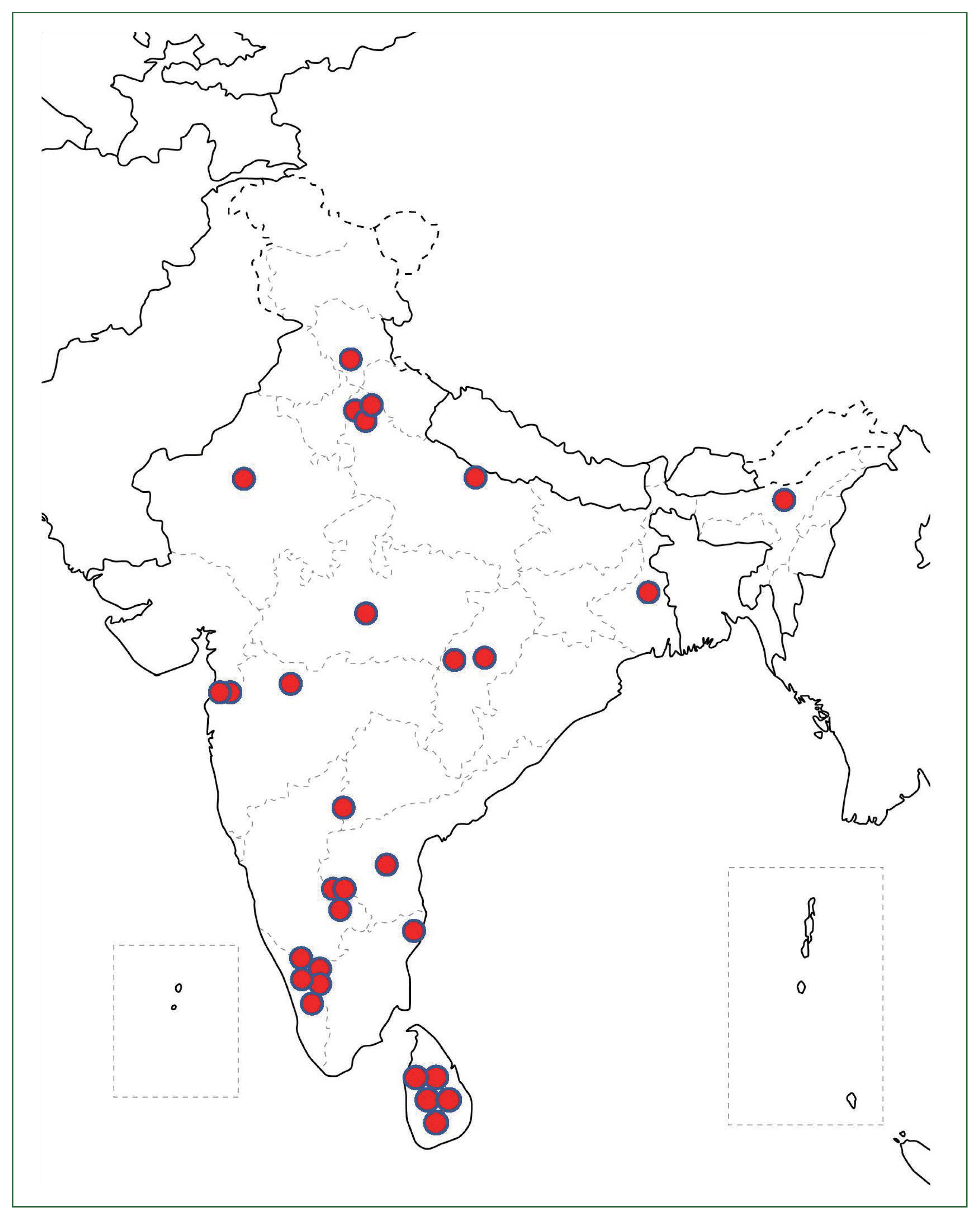
26]. Their mean age was 29.3 years-old ranging from 4 to 60 years-old. No obvious gender difference was observed with the M:F ratio of 13:12. Their geographical distribution together with 5 cases in Sri Lanka (details are given below) is shown in
Fig. 1. In addition to those indigenous cases listed in
Table 1, there is a case report of cerebral sparganosis in an American salesman who frequently visit India on his business [
27]. Conversely, a case of cerebral sparganosis in an Indian man living several years in USA was reported [
28].
In Sri Lanka, Wijesundera et al. [
29] first reported 2 cases of cutaneous sparganosis presented as non-tender subcutaneous lumps; one case is a 45 years-old male with left-groin lesion, and the other is a 28 years old female with left-upper arm lesion. Subsequently, Dissanike et al. [
30] added 2 more cases of cutaneous sparganosis in which a plerocercoid larva (sparganum), probably of
Spirometra sp., was successfully removed from the anterior abdominal wall of 2 patients (a 40-year-old man and a 23-year-old woman) in Colombo. In addition, Alibhoy et al. [
31] reported a case of cerebral sparganosis in a 5-year-old boy in Sri Lanka.
A couple of review articles on parasitic zoonoses in Nepal mentioned about the incidence of potential sparganosis in Nepal without referring to actual cases [
32,
33]. A case of breast sparganosis in a 57-year-old Nepalese woman living in UK was reported [
34]. She was born in Nepal and had moved to UK 12 years previously, but she visited Nepal 1 year before the onset of the disease. Although Sah et al. [
35] reported 4 asymptomatic ocular helminthiasis and 3 of them were possibly be an infection with sparganum of
Spirometra species, the size of the worms in the eyes appeared to be too small as a sparganum.
Situation of sparganosis in Bangladesh is similar to that in Nepal. Although
Spirometra sp. was found in wild animals [
36], actual indigenous human cases have not yet been reported. A case of cerebral sparganosis in a Bangladesh man was reported from Switzerland [
37].
Situation of human sparganosis in the Middle East is similar to that observed in Nepal and Bangladesh. Thus,
Spirometra sp. tapeworms have been found in mammalian final hosts [
38–
42] and/or amphibian/reptile intermediate hosts [
43] in this area. However, until very recently, human sparganosis cases have not been reported from Middle East. While we are preparing this manuscript, a case of hand palm sparganosis in a 14-year-old girl was reported from Egypt with morphological and genetic identification of 2 spargana as
Spirometra erinaceieuropaei [
44].
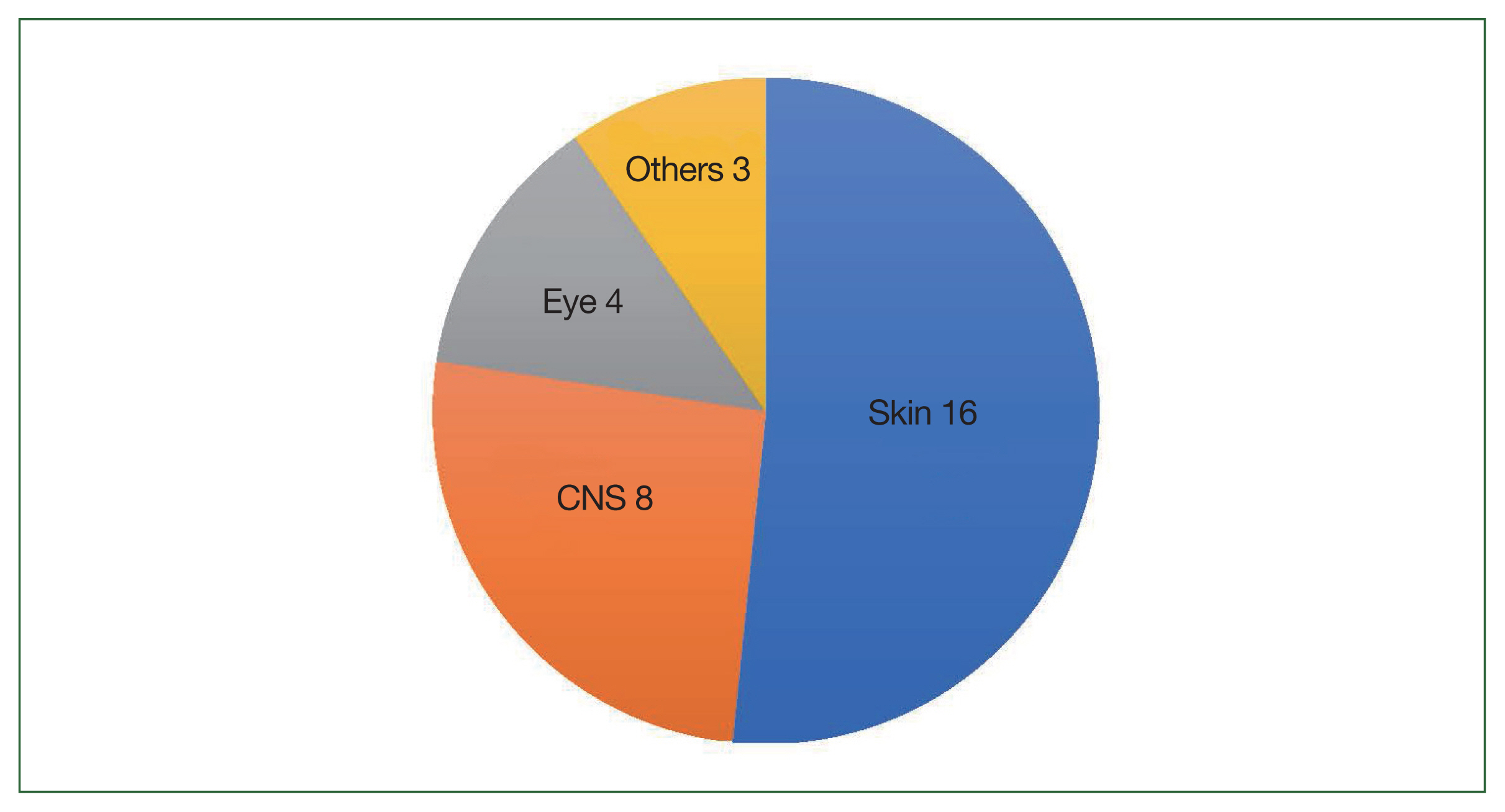
After an extemsive literature review, we could find 25 cases in India, 5 cases in Sri Lanka, and 1 case in Egypt. The affected sites of all the patients are summarized in
Fig. 2; among 31 sparganosis cases in the Indian subcontinent and Middle East, 16 cases are cutaneous sparganosis followed by 8 cases of CNS sparganosis (incl. 1 case of spinal lesion) and 4 cases of ocular sparganosis. In one case each, a worm (sparganum) was found in perinephritic abscess, the urinary tract and the liver.
Discussion
The genus
Spirometra consisting of several species is a medium sized tapeworm parasitizing the intestine of carnivorous mammalian hosts. This tapeworm is zoonotic and when humans ingest their larval stage in the intermediate or paratenic hosts, the larvae migrate into various organs/tissues to cause acute to chronic inflammatory changes. This tapeworm is cosmopolitan and distribute worldwide. High endemicity of this disease in humans in East and Southeast Asia is related to the traditional eating habits where people consume uncooked/undercooked meats of intermediate/paratenic hosts for
Spirometra, e.g., amphibians, reptiles or chickens. Thus, in those endemic areas, sparganosis is considered principally a food-borne parasitic zoonosis [
2–
5]. In addition, in some areas, frog meat has been used as a poultice for eye diseases in the traditional medicine [
2–
4]. In contrast, in this study, the most likely source of infection with sparganum in the Indian subcontinent and the Middle East is assumed to be ingestion of the infected first intermediate host, cyclops in water, and thus the disease is considered a water-borne disease [
7,
15,
44].
In terms of the causative
Spirometra species, most of the case reports listed here mentioned it at the genus level and not intended to identify the species. Exception is the one recent case report from Egypt, in that the parasite retrieved from the patient was identified as
S. erinaceieuropaei by the molecular method. Although Datta et al. [
6] identified the worm as
S. mansoni, morphological/morphometrical data were not provided. Bharucha et al. [
12] also mentioned the worm from the brain of the patient as
S. mansoni without solid morphological evidences of the worm. In a case of American salesman frequently visited India, the worm from his brain was identified as
S. mansonoides [
27]. Since this species is distributed only in the Americas, whether he was infected in USA or in India remains unknown. Molecular identification of the worm is necessary for such a case. Recently, based on the molecular data, the taxonomic classification and geographical distribution has been drastically changed [
45,
46]. For example,
S. erinaceieuropaei was considered the most common zoonotic
Spirometra species in East and Southeast Asian countries. However, this name is now applicable only to the European isolates [
45]. For the major Asian isolates previously named
S. erinaceieuropaei, Yamasaki et al. [
46] recommended to use
S. mansoni as the valid name. Together with this proposal, they reported the discovery of new
Spirometra species,
S. asiana sp. nov. adults from dogs and plerocercoids from wild boars in Japan and its zoonotic nature was proven by the molecular data base search [
46]. As the rare human cases, infections with
Spirometra decipiens [
47] and
S. ranarum [
48] have been reported. Since validity of those 2 species are still under debate, more extensive molecular epidemiological study is necessary to identify the causative agent(s) for human sparganosis. In particular, the Indian subcontinent and the Middle East are the cross-passing place of animals and their parasites, exact identification of the causative agents of sparganosis in this area is extremely interesting to elucidate the diversification of
Spirometra species.
Notes
-
Author contributions
Conceptualization: Nawa Y
Data curation: Nawa Y, Tanaka M, Yoshikawa M
Formal analysis: Nawa Y, Tanaka M, Yoshikawa M
Investigation: Nawa Y, Tanaka M, Yoshikawa M
Project administration: Nawa Y
Validation: Nawa Y, Tanaka M, Yoshikawa M
Visualization: Nawa Y, Tanaka M
Writing – original draft: Nawa Y
Writing – review & editing: Tanaka M, Yoshikawa M
-
We have no conflict of interest related to this work.
Acknowledgment
This study is a literature survey and is not a subject of ethical approval.
Fig. 1Geographical distribution of sparganosis patients in the Indian subcontinent.

Fig. 2The affected organs of the sparganosis patients in the Indian subcontinent.

Table 1Human sparganosis cases in the Indian subcontinent and the Middle East
Table 1
|
No. |
Year |
Age |
Sex |
Affected site |
Locality |
Ref. |
|
India |
|
1 |
1982 |
40 |
M |
Skin (chest, right) |
Jodhpur |
[6] |
|
2 |
1989 |
28 |
M |
Eye |
Delhi |
[8] |
|
3 |
1993 |
24 |
F |
Skin |
Bombey |
[9] |
|
4 |
1996 |
25 |
F |
Brain |
Delhi |
[10] |
|
5 |
1998 |
38 |
M |
Brain |
Bangalore |
[11] |
|
6 |
1998 |
10 |
F |
Spinal cord |
|
|
|
7 |
1999 |
18 |
M |
Brain |
Mumbai |
[12] |
|
8 |
2003 |
22 |
M |
Brain |
Hyderabad |
[13] |
|
9 |
2006 |
50 |
M |
Eye (Conjunctiva) |
West Bengal |
[14] |
|
10 |
2007 |
30 |
M |
Eye (Conjunctiva) |
Chennai |
[15] |
|
11 |
2008 |
29 |
F |
Brain |
Bangalore |
[16] |
|
12 |
2011 |
25 |
M |
Peri-renal fluid drainage |
Uttar Pradesh |
[17] |
|
13 |
2012 |
1.5 |
F |
Liver |
Chandigarh |
[18] |
|
14 |
2014 |
31 |
M |
Skin (axillary) |
Andhra Pradesh |
[19] |
|
15 |
2013 |
9 |
M |
Skin (inguinal) |
Kerala |
[20] |
|
16 |
2010 |
35 |
F |
Skin (abdominal wall) |
Calicut, Kerala |
[21] |
|
17 |
2012 |
38 |
F |
Skin (calf, left) |
|
|
|
18 |
2013 |
30 |
F |
Skin (femoral triangle, left) |
|
|
|
19 |
2015 |
32 |
F |
Skin (thigh, right) |
|
|
|
20 |
2015 |
32 |
M |
Eye (Conjunctiva) |
Assam |
[22] |
|
21 |
2015 |
50 |
M |
Skin (cheek) |
Chattisgarh |
[23] |
|
22 |
2016 |
28 |
F |
Skin (breast) |
Maharashtra |
[24] |
|
23 |
2018 |
30 |
F |
Urinary tract |
Chattisgarh |
[25] |
|
24 |
2021 |
4 |
F |
Skin (r-foot) |
Delhi |
[26] |
|
25 |
2023 |
60 |
M |
Brain, incl. review of 20 cases |
Bhopal |
[7] |
|
|
Sri Lanka |
|
26 |
1996? |
45 |
M |
Skin (groin, left) |
Kegalle |
[29] |
|
27 |
1996 |
28 |
F |
Skin (upper arm, left) |
Ragama |
|
|
28 |
1999 |
40 |
M |
Skin |
Kurunegala |
[30] |
|
29 |
2001 |
23 |
F |
Skin (abdominal wall) |
Karutala |
|
|
30 |
2005 |
13 |
M |
Brain |
Colombo |
[31] |
|
|
Egypt |
|
31 |
2023 |
14 |
F |
Skin (hand palm, right) |
Qualyubia Governorate |
[44] |
References
- 1. Liu W, Gong T, Chen S, Liu Q, Zhou H, et al. Epidemiology, diagnosis, and prevention of sparganosis in Asia. Animals 2022;12(12):1578.
https://doi.org/10.3390/ani12121578
- 2. Kim JG, Ahn CS, Sohn WM, Nawa Y, Kong Y. Human sparganosis in Korea. J Korean Med Sci 2018;33(44):e273.
https://doi.org/10.3346/jkms.2018.33.e273
- 3. Yoshikawa M, Ouji Y, Nishiofuku M, Ishizaka S, Nawa Y. Sparganosis cases reported in Japan in the recent decade, 2000–2009. Clin Parasitol 2010;21:33-36. (in Japanese).
- 4. Anantaphruti MT, Nawa Y, Vanvanitchai Y. Human sparganosis in Thailand: an overview. Acta Tropica 2011;118(3):171-176.
http://doi.org/10.1016/j.acta.tropica.2011.03.011
- 5. Boonyasiri A, Cheunsuchon P, Suputtamongkol Y, Yamasaki H, Sanpool O, et al. Nine human sparganosis cases in Thailand with molecular identification of causative parasite species. Am J Trop Med Hyg 2014;91(2):389.
http://doi.org/10.4219/ajtmh.14.0218
- 6. Datta KK, Datta SP, Sharma RS, Goyal SL. Sparganosis. J Indian Med Assoc 1982;79(5–6):78-80.
- 7. Kaur S, Shukla P. Cerebral sparganosis masquerading brain neoplasm: a rare incidental case. Indian J Med Microbiol 2023;41:101-103.
https://doi.org/10.1016/j.ijmmb.2022.10.009
- 8. Sen DK, Muller R, Gupta VP, Chilana JS. Cestode larva (Sparganum) in the anterior chamber of the eye. Trop Geogr Med 1989;41(3):270-273.
- 9. Deshpande VV. Subcutaneous sparganosis--a rare infection in man. J Assoc Physic India 1993;41(10):685.
- 10. Sharma MC, Sudha K, Rathore A, Sarkar C, Gaikwad S, et al. Two rare parasites of the human brain--Gnathostoma spinigerum and sparganum (Spirometra). J Assoc Physic India 1996;44(11):824-828.
- 11. Kudesia S, Indira DB, Sarala D, Vani S, Yasha TC, et al. Sparganosis of brain and spinal cord: unusual tapeworm infestation (report of two cases). Clin Neurol Neurosurg 1998;100(2):148-152.
- 12. Bharucha NE, Bhagwati AN, Kanphade MM. Epilepsy and solitary lesions. Surg Neurol 1999;52(2):208-209.
- 13. Sundaram C, Prasad VS, Reddy JJ. Cerebral sparganosis. J Assoc Physic India 2003;51:1107-1109.
- 14. Subudhi BN, Dash S, Chakrabarty D, Mishra DP, Senapati U. Ocular sparganosis. J Indian Med Assoc 2006;104(9):529-530.
- 15. Mukherjee MS, Biswas J, Raman M. Subconjunctival larva migrans caused by spraganum. Ind J Ophthalmol 2007;55(3):242-243.
https://doi.org/10.4103/0301-4738.31959
- 16. Rengarajan S, Nanjegowda N, Bhat D, Mahadevan A, Sampath S, et al. Cerebral sparganosis: a diagnostic challenge. Br J Neurosurg 2008;22(6):784-786.
https://doi.org/10.1080/02688690802088073
- 17. Duggal S, Mahajan R, Duggal N, Hans C. Case of sparganosis: a diagnostic dilemma. Indian J Med Microbiol 2011;29(2):183-186.
https://doi.org/10.4103/0255-0857.81789
- 18. Khurana S, Appannanavar S, Bhatti HS, Verma S. Sparganosis of liver: a rare entity and review of literature. BMJ Case Rep; 2012. 2012:bcr2012006790
https://doi.org/10.1136/bcr-2012-006790
- 19. Anusha AM. Subcutaneous sparganosis: a rare case report. IOSR J Dent Med Sci 2014;13(6):6-8.
- 20. Sabu L, Lakshmanan B, Devada K, Sundaresh Kumar P. Occurrence of human sparganosis in Kerala. J Parasitic Dis 2015;39(4):777-779.
https://doi.org/10.1007/s12639-014-0421-y
- 21. Sudarsana J, Mampilly N, Rasalam N. Sparganosis-not uncommon in Calicut, Kerala. BMH Med J 2016;3(1):10-14.
- 22. Nath R, Gogoi R. Ocular sparganosis from Assam. Trop Parasitol 2015;5(1):64-67.
https://doi.org/10.4103/2229-5070.149930
- 23. Agrawal DM, Agrawal DE, Murthy DR. Sparganosis –a rare case report. Int J Med Res Rev 2015;3(4):448-450.
https://doi.org/10.17511/ijmrr.2015.i4.081
- 24. Shah BC, Degloorkar S. Breast sparganosis: a rare cause of breast lump. J Case Rep 2016;6(4):534-536.
https://doi.org/10.17659/01.2016.0130
- 25. Trupti B, Shirish N, Maneesha P, Santosh A. An unusual case of urinary sparganosis in the Indian subcontinent. Indian J Urol 2018;34(2):158-160.
https://doi.org/10.4103/iju.IJU_273_17
- 26. Sharma S, Mahajan RK, Ram H, Karikalan M, Achra A. Sparganosis mimicking a soft-tissue tumor: a diagnostic challenge. Trop Parasitol 2021;11(1):49-51.
https://doi.org/10.4103/tp.TP_40_20
- 27. Mitchell A, Scheithauer BW, Kelly PJ, Forbes GS, Rosenblatt JE. Cerebral sparganosis. Case report. J Neurosurg 1990;73:147-150.
https://doi.org/10.3171/jns.1990.73.1.0147
- 28. Holodniy M, Almenoff J, Loutit J, Steinberg GK. Cerebral sparganosis: case report and review. Rev Infect Dis 1991;13(1):155-159.
https://doi.org/10.1093/clinids/12.5.155
- 29. Wijesundera MS, Ratnatunga N, Kumarasinghe MP, Dissanaike AS. First reports of subcutaneous sparganosis in Sri Lanka. Ceylon Med J 1997;42(1):30-32.
- 30. Dissanaike AS, Anthonis PR, Sherifdeen AH, Ihalamulla RL, Karunaweera ND. Two more cases of sparganosis from Sri Lanka. Ceylon Med Sci 2001;44(1):19-22.
https://doi.org/10.4038/cjms.v44i1.4869
- 31. Alibhoy A, Perera F, Fernando R. Cerebral sparganosis: a case report from Sri Lanka. J Neurol Sci 2005;238:S468.
- 32. Rai SK. Zoonotic parasitic diseases in Nepal. Proceedings of the Parasitic Zoonoses in Asia-Pacific Regions 2012. Kobe, Japan: 2012; 10-14.
- 33. Devleesschauwer B, Ale A, Torgerson P, Praet N, de Noordhout C, et al. The burden of parasitic zoonoses in Nepal: a systematic review. PLoS Negl Trop Dis 2014;8(1):e2634.
https://doi.org/10.1371/journal.pntd.0002634
- 34. Blundell S, Deshmukh M, McGregor A. A painful breast mass. Clin Infect Dis 2022;75(12):2275-2277.
https://doi.org/10.1093/cid/ciac250
- 35. Sah R, Khatri A, Kharel R, Kc H, Rabaan AA, et al. Case report: management of dead intraocular helminth parasites in asymptomatic patients. Am J Trop Med Hyg 2020;103(2):719.
https://doi.org/10.4269/ajtmh.20-0218
- 36. Nath TC, Eom KS, Choe S, Hm S, Islam S, et al. Insight into one health approach: endoparasite infections in captive wildlife in Bangladesh. Pathogens 2021;10(2):250.
https://doi.org/10.3390/pathogens.10020250
- 37. Gonzenbach RR, Kong Y, Beck B, Buck A, Weller M, et al. High-dose praziquantel therapy for cerebral sparganosis. J Neurol 2013;260:1423-1425.
https://doi.org/10.1007/s00415-013-6901-7
- 38. Badri M, Eslahi AV, Majidiani H, Pirestani M.
Spirometra erinaceieuropaei in a wildcat (Felis silvestris) in Iran
. Vet Parasitol Reg Stud Rep 2017;10:58-61.
https://dx.doi.org/10.1016/j.vprsr.2017.08.004
- 39. Beiromvand M, Rafiei A, Razmjou E, Maraghi S. Multiple zoonotic helminth infections in domestic dogs in a rural area of Khuzestan Province in Iran. BMC Vet Res 2018;14(1):1-7.
https://doi.org/10.1186/s12917-018-1529-6
- 40. Amouei A, Jahandar H, Daryani A, Sharif M, Sarvi S, et al. Carnivores as important reservoirs of intestinal helminthic infections in Mazandaran Province, Northern Iran. Iran J Parasitol 2018;13(2):251-257.
- 41. Al-Obaidi QT. Prevalence of internal helminthes in stray cats (Felis Catus) in Mosul City, Mosul-Iraq. J Animal Vet Adv 2012;11(15):2732-2736.
https://doi.org/10.3923/javaa.2012.2732.2736
- 42. Vafae Eslahi A, Kia EB, Mobedi I, Sharifdini M, Badri M, et al. Road killed carnivores illustrate the status of zoonotic helminths in Caspian Sea Littoral of Iran. Iran J Parasitol 2017;12(2):230-235.
- 43. Yildirimhan HS, Bursey CR, Goldberg SR. Helminth parasites of the grass snake, Natrix natrix, and the dice snake, Natrix tessellata (Serpentes: Colubridae), from Turkey. Comp Parasitol 2007;74(2):343-354.
https://doi.org/10.1654/4285.1
- 44. Omar HM, Fahmy M, Abuowarda M. Hand palm sparganosis: morphologically and genetically confirmed Spirometra erinaceieuropaei in a fourteen-year-old girl, Egypt. J Parasitic Dis 2023;47:859-864.
https://doi.org/10.1007/s12639-023-01623-5
- 45. Kuchta R, Kołodziej-Sobocińska M, Brabec J, Młocicki D, Sałamatin R, et al. Sparganosis (Spirometra) in Europe in the molecular era. Clin Infect Dis 2021;72(5):882-890.
https://doi.org/10.1093/cid/ciaa1036
- 46. Yamasaki H, Sugiyama H, Morishima Y, Kobayashi H. Description of Spirometra asiana sp. nov.(Cestoda: Diphyllobothriidae) found in wild boars and hound dogs in Japan. Parasitol Int 2024;98:102798.
https://doi.org/10.1016/j.parint.2023.102798
- 47. Jeon HK, Park H, Lee D, Choe S, Kim KH, et al. Human infections with Spirometra decipiens plerocercoids identified by morphologic and genetic analyses in Korea. Korean J Parasitol 2015;53(3):299-305.
https://doi.org/10.3347/kjp.2015.53.3.299
- 48. Saksirisampant W, Eamudomkarn C, Jeon HK, Eom KS, Assavapongpaiboon B, et al. Ocular sparganosis: the first report of Spirometra ranarum in Thailand. Korean J Parasitol 2020;58(5):577-581.
https://doi.org/10.3347/kjp.2020.58.5.577