Abstract
To know the prevalence of Enterobius vermicularis infection and what are the most important risk factors, we evaluated the incidence and risk factors of enterobiasis among children attended in kindergartens in Busan metropolitan city, Republic of Korea. A total of 1,674 children from 21 kindergartens in 11 of 16 autonomous districts of Busan were evaluated for E. vermicularis infection by the cellotape anal swab technique. The overall egg-positive rate for E. vermicularis was 10.7% (179/1,674), and the prevalence of enterobiasis in each kindergarten ranged between 0% and 32.4%. There was an increasing tendency of the egg positive rate according to the population density; the higher the population density communities had, the higher egg-positive rate for E. vermicularis was detected (P = 0.001). Among personal hygiene factors involving children, thumb-sucking (P = 0.036) and fingernail-trimming (P = 0.024) were highly associated with enterobiasis. In addition, taking anthelmintic medications against E. vermicularis infection was strongly associated with enterobiasis (P = 0.014). Moreover, parents' knowledge of enterobiasis was correlated significantly with the incidence of enterobiasis of their children (P = 0.006). In conclusion, we need to consider not only personal hygiene but also parents' knowledge about enterobiasis as a factor in order to develop new strategies for elimination or to complete reduction of enterobiasis in Korea.
-
Key words: Enterobius vermicularis, risk factor, cellotape anal swab, health education
INTRODUCTION
Enterobius vermicularis (the pinworm) inhabits at least 400 million people; this fact is, perhaps, less surprising than the fact that practically nothing is currently being done to eliminate infections [
1]. Part of the reason for this was that the symptoms of enterobiasis are not fatal, and it can be readily transmitted via direct contact between infected and uninfected persons. Although the majority of infections are asymptomatic, they can induce bothersome symptoms in some cases, including an itching sensation and irritation in the perianal area, along with mental distraction. Very rarely, pinworms will penetrate into the wall of the colon, in the retrocaecal tissues, and on the peritoneum [
2]. Commonly, live worms wander into the vulva, where they remain for several days, and cause vulval itching associated with scanty vaginal discharge and mild irritation [
3,
4].
The prevalence of enterobiasis has been decreased every year in Korea. The egg positive rate of
E. vermicularis was 0.6% in the general population, according to a nationwide survey of intestinal parasites conducted in 2004 by The Ministry of Health and Welfare, Korea, and Korea Association of Health Promotion. Nevertheless, in primary school children, a relatively high egg-positive rate (from 7.8% to 18.5%) has been reported in both urban and rural areas of Korea [
5-
7]. Since 2004, however, we have not found any literature about the prevalence of enterobiasis in Korea, especially there have been no reports on the infection rates of
E. vermicularis in Busan metropolitan city up to now. Recently, the number of young children being cared for at a kindergarten is increasing because their mothers may be employed, or parents want their children to play and be educated in a well-organized educational system. Therefore, the majority of
E. vermicularis infections in children probably occurs in daycare centers [
7].
Many studies have been conducted to explore the risk factors for enterobiasis. The main risk factors are associated with indoor living conditions, including personal sanitary and close contact with other people, as pinworms spread mainly indoors directly from one human to another. Although infected children are given anthelmintics after a survey, reinfection is strong and very rapid. For this reason, the prevalence of enterobiasis has not shown a decrease in recent years. It is needed to consider health educational aspects, in particular, parent's correct knowledge about enterobiasis.
Currently, little information is available regarding the prevalence and possible risk factors of enterobiasis among kindergarten children in metropolitan cities in Korea. In this study, we evaluated the incidence and risk factors of enterobiasis in 11 of 16 autonomous districts of the metropolitan city of Busan. Suggestions were made to reduce the prevalence of enterobiasis in this study.
MATERIALS AND METHODS
Survey
For recruitment, the letter that contained information about the nature, significance, and objectives of the study, copies of a questionnaire, a guide for swab examination, and a consent form were sent to 302 directors of kindergartens registered in the Busan Association of Kindergartens. Among them, 21 kindergartens from 11 of the 16 communities in Busan agreed to participate in this study (
Fig. 1). This study was presented by the researcher to the directors of each kindergarten, and then the directors sent the parent's consent form, letter of information, and a questionnaire. Of 3,194 parents, 1,695 (53.1%) agreed to participate in this study. Among the 1,695 children aged 1-7 years, 21 children for whom more than 10% of the relevant survey data were missing were excluded. Ultimately, the data from 1,674 (98.8%) children examined for
E. vermicularis infection using the cellotape anal swab technique were collected and analyzed in this study.
A questionnaire was provided to the parents of each child asking them about their child's personal hygiene, sanitary environment, and the family's socioeconomic status and general knowledge of enterobiasis.
Statistical analysis
Data were analyzed using SPSS for Windows, version 14 (SPSS, Chicago, Illinois, USA). The association of the egg-positive rate of E. vermicularis and factors involving children and their family were analyzed using χ2 test and Fisher's exact test. The correlation between the rate of E. vermicularis infection and population density was analyzed using Pearson's correlations. Also, the correlation between E. vermicularis infection rates and knowledge of E. vermicularis infection was analyzed using Pearson's correlations.
RESULTS
The overall egg-positive rate for
E. vermicularis was 10.7% (179/1,674), and the prevalence of enterobiasis in each kindergarten ranged between 0% and 32.4%. There was significant difference of the egg-positive rate for
E. vermicularis according to the population densities of the community (
P = 0.001), with egg-positive rate of 4.7% for communities of not more than 5,000 people per km
2, 9.1% for 5,001-10,000, 10.8% for 10,001-15,000, and 16.5% for not less than 15,001 people per km
2. A significantly close correlation was detected between the
E. vermicularis infection rate and population density (
P = 0.020) (
Table 1).
Table 2 shows the personal hygiene and other factors that may potentially be associated with the egg-positive rates of
E. vermicularis. In general, the prevalence of enterobiasis increased with advancing age; however, this was not significant. The infection rate was significantly higher in boys than in girls. The educational level of the parents was not found to be associated with enterobiasis (data not shown). Among several personal hygiene factors, thumb-sucking and fingernail-trimming were associated with enterobiasis. The children with the habit of scratching around the anus were more infected by
E. vermicularis than those who did not have this habit; however, this was not significant. The cleanliness of the home environment was not found to be a significant risk factor. On the screening day, children who had received anthelmintic medication within 1 month were not infected by
E. vermicularis, but after 1 month, the children might be readily reinfected by the worms. Also, about a half of children has not taken anthelmintic medications.
We evaluated the correlation between the parents' knowledge regarding enterobiasis and the incidence of enterobiasis in their children using a questionnaire (
Table 3). The children of the parents with the higher of correct answers on the survey evidenced lower rates of
E. vermicularis infection (
P = 0.006). Scores of items (No. 1, 2) about
E. vermicularis life cycle were very low (27.5-31.8), also scores of items (No. 7, 8) about treatment methods (60.8-68.6) were comparatively lower than those of personal hygiene (52.1-96.9). These results show although most of parents knew that good personal hygiene can help to reduce the chances of becoming infected by
E. vermicularis, they did not know well about the correct methods for treatment of
E. vermicularis infection.
DISCUSSION
Although enterobiasis is generally considered to be a nuisance rather than a fatal disease, the level of morbidity is significant, particularly in children. Therefore, this worm is one of the most frequently encountered and ubiquitous nematodes. Although enterobiasis can be readily cured by anthelmintic medications, the prevalence of this infection has not diminished over the past decade [
5,
7-
9].
Why has the infection rate of
E. vermicularis not been reduced? In this study, we identified some important factors in enterobiasis; personal hygiene involving children, population density, repeated medications, and accurate knowledge of the infection. Firstly, personal hygiene factors are closely associated with
E. vermicularis infection. Previous reports suggested that inadequate personal hygiene can increase the risk of enterobiasis among primary school children. In addition, factors significantly associated with enterobiasis include playing on the floor, nail biting, failure to wash hands before meals, and living in non-apartment dwellings [
10]. In our study, children with the habits of thumb-sucking or fingernail trimming evidenced significantly higher rates of
E. vermicularis infection than those who did not have these habits.
Secondly, anthelmintic therapy is one of the most effective tools for eradication of enterobiasis; whether it is correctly treated or not (group therapy and repeated treatment with anthelmintic medications). In this study, just 1 among 21 kindergartens scheduled anthelmintic medication programs in which all children and teachers in a kindergarten take the medication at the same time every 6 months, keeping repeated treatment with the medicines after 2 weeks (personal communication). Therefore, the children in the kindergarten have no enterobiasis; although other kindergartens, where located same an administrative district with similar environments with the infection free kindergarten, have higher-than-average rates of
E. vermicularis infection (
Fig. 1). In addition, approximately a half of children have never taken anthelmintic medicine against parasites, including the pinworm. Although the other half of the children have an experience to take an anthelmintic medicine at least once a year, the medication methods was not likely to be correct (discussed in below). These results provide a clue for why the incidence of enterobiasis has not decreased further. Each child takes an anthelmintic medicine on different days of the year the children can readily become reinfected with
E. vermicularis within 1 month after beginning of the medication. Because the medicine for enterobiasis is not effective to eggs and larval stages of
E. vermicularis, recent infection before treatment could not be cured by 1 time medication. Therefore, the infected children should take the medicine 1 more time after the first treatment [
11,
12]. Interestingly, in 1 family, 1 brother had enterobiasis but the other brother did not have enterobiasis, although both regularly took anthelmintics every 6 months. This result shows that reinfection of
E. vermicularis occurs very commonly in a contaminated kindergarten class, rather than at home. Additionally, some previous reports have suggested that the environments of daycare centers constitute a crucial factor in enterobiasis, especially as compared to personal hygiene factors [
7,
13,
14].
Finally, parents were asked questions regarding their knowledge of enterobiasis, using a structured questionnaire. The accurate response rate for
E. vermicularis infection characteristics was 67.6%. The overall egg-negative group was more knowledged than the egg-positive group, especially on items related to treatment of helminthic infections (
Table 3). As most parents know like that anthelmintic medication could easily cure every intestinal helminthic infection, including
E. vermicularis, by just 1 time treatment. Therefore, they think that their children may take just 1 time medication. They have no idea for the necessity of re-treatment against pinworm infections, because they have known that most pinworm infections are not fatal and that they can eliminate the worms whenever they want. Our results suggested that parents' correct knowledge about enterobiasis is one of the most important factors for eradication of
E. vermicularis. Because parents have the greatest influence on their child's habits, we need to assess whether parents have correct knowledge about enterobiasis, for instance, how often they have to take the medicine.
Directors and teachers of the kindergartens included in this study hesitated to provide information regarding the characteristics of a kindergarten, such as the numbers and times that the classroom was cleaned, the times the toys were washed, the numbers of children in a class, and so on. Therefore, we were unable to evaluate the potential risk factors associated with the kindergartens assessed in this study. However, it is necessary to identify environmental risk factors for enterobiasis, as the majority of E. vermicularis infections might be transmitted in those places.
In conclusion, enterobiasis is commonly detected in kindergarteners in Busan. In addition, a half of the children have never taken any medicine for treatment of enterobiasis, and most of the other half has been treated but without correct medication guidelines. Therefore, it is necessary not only to do mass screening and regular group therapy for children with correct medicationmethods, but also to develop pinworm eradiation programs, such as health education programs (about enterobiasis) for the parents, in order to control E. vermicularis infection in Korea.
ACKNOWLEDGEMENTS
This work was supported for 2 years by a Pusan National University Research Grant.
References
- 1. Hopkins DR. Homing in on helminths. Am J Trop Med Hyg 1992;46:626-634.
- 2. McDonald GS, Hourihane DO. Ectopic Enterobius vermicularis. Gut 1972;13:621-626.
- 3. Chung DI, Kong HH, Yu HS, Kim J, Cho CR. Live female Enterobius vermicularis in the posterior fornix of the vagina of a Korean woman. Korean J Parasitol 1997;35:67-69.
- 4. Deshpande AD. Enterobius vermicularis live adult worms in the high vagina. Postgrad Med J 1992;68:690-691.
- 5. Kang S, Jeon HK, Eom KS, Park JK. Egg positive rate of Enterobius vermicularis among preschool children in Cheongju, Chungcheongbuk-do, Korea. Korean J Parasitol 2006;44:247-249.
- 6. Park JH, Han ET, Kim WH, Shin EH, Guk SM, Kim JL, Chai JY. A survey of Enterobius vermicularis infection among children on western and southern coastal islands of the Republic of Korea. Korean J Parasitol 2005;43:129-134.
- 7. Song HJ, Cho CH, Kim JS, Choi MH, Hong ST. Prevalence and risk factors for enterobiasis among preschool children in a metropolitan city in Korea. Parasitol Res 2003;91:46-50.
- 8. Kim BJ, Yeon JW, Ock MS. Infection rates of Enterobius vermicularis and Clonorchis sinensis of primary school children in Hamyang-gun, Gyeongsangnam-do (province), Korea. Korean J Parasitol 2001;39:323-325.
- 9. Kim BJ, Lee BY, Chung HK, Lee YS, Lee KH, Chung HJ, Ock MS. Egg positive rate of Enterobius vermicularis of primary school children in Geoje island. Korean J Parasitol 2003;41:75-77.
- 10. Sung JF, Lin RS, Huang KC, Wang SY, Lu YJ. Pinworm control and risk factors of pinworm infection among primary-school children in Taiwan. Am J Trop Med Hyg 2001;65:558-562.
- 11. Cho SY, Ahn YR, Ryang YS, Seo BS. Evaluation of anthelmintic treatment of Enterobius vermicularis infection in highly endemic population by prolonged observation. Korean J Parasitol 1977;15:100-108.
- 12. Cho SY, Kang SY, Kim SI, Song CY. Effect of anthelmintics on the early stage of Enterobius vermicularis. Korean J Parasitol 1985;23:7-17.
- 13. Cook GC. Enterobius vermicularis infection. Gut 1994;35:1159-1162.
- 14. Norhayati M, Hayati MI, Oothuman P, Azizi O, Fatmah MS, Ismail G, Minudin YM. Enterobius vermicularis infection among children aged 1-8 years in a rural area in Malaysia. Southeast Asian J Trop Med Public Health 1994;25:494-497.
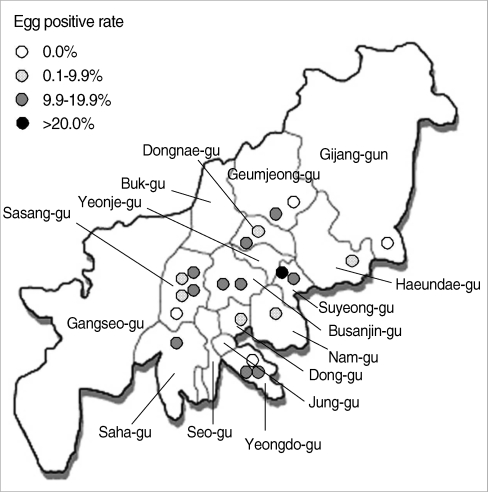
Fig. 1Distribution of surveyed areas and egg positive rates for Enterobius vermicularis infections in Busan Metropolitan City.

Table 1.
Enterobius vermicularis egg positive rates in surveyed areas
Table 1.
|
Surveyed area |
Population density (no. people/km2) |
No. of surveyed kindergarten (No. of samples) |
Egg positive rate (%) |
|
Dong-gu |
11,246 |
1 (185) |
8.6 |
|
Yeongdo-gu |
7,651 |
3 (95) |
13.7 |
|
Busanjin-gu |
13,830 |
2 (222) |
13.1 |
|
Dongnae-gu |
16,773 |
2 (179) |
9.5 |
|
Nam-gu |
11,657 |
1 (18) |
5.5 |
|
Haeundae-gu |
7,865 |
1 (42) |
9.5 |
|
Saha-gu |
9,093 |
1 (147) |
13.6 |
|
Geumjeong-gu |
4,063 |
2 (59) |
6.8 |
|
Suyeong-gu |
17,501 |
2 (137) |
25.5 |
|
Sasang-gu |
7,742 |
5 (564) |
7.1 |
|
Gijang-gun |
368 |
1 (26) |
0.0 |
|
Total |
4,766 |
21 (1,674) |
10.7 |
Table 2.Egg positive rate of Enterobius vermicularis among children according to their family factors
Table 2.
|
Variables |
Number of positive |
Number of examined |
Egg positive rate (%) |
P value |
Variables |
Number of positive |
Number of examined |
Egg positive rate (%) |
P value |
|
Age (years) |
|
|
|
0.274 |
Scratching around the anus |
|
|
|
0.108 |
|
≤3 |
6 |
106 |
5.7 |
|
Yes |
84 |
682 |
12.3 |
|
|
4 |
31 |
303 |
10.2 |
|
No |
95 |
977 |
9.7 |
|
|
5 |
59 |
556 |
10.6 |
|
Subtotal |
179 |
1,659 |
10.8 |
|
|
≥6 |
81 |
681 |
11.9 |
|
Cleaning of home |
|
|
|
0.120 |
|
Subtotal |
177 |
1,646 |
10.8 |
|
1/day |
116 |
1,151 |
10.1 |
|
|
Gender |
|
|
|
0.001 |
2-3/week |
63 |
494 |
12.8 |
|
|
Boys |
116 |
887 |
13.1 |
|
Subtotal |
179 |
1,645 |
10.9 |
|
|
Girls |
63 |
786 |
8.0 |
|
Cleaning of bedding |
|
|
|
0.548 |
|
Subtotal |
179 |
1,673 |
10.7 |
|
≤7 |
55 |
564 |
9.8 |
|
|
Housing |
|
|
|
0.571 |
≥8 |
110 |
1,020 |
10.8 |
|
|
Apartment |
135 |
1,216 |
11.1 |
|
Subtotal |
165 |
1,584 |
10.4 |
|
|
Private residence |
28 |
251 |
11.2 |
|
Family size |
|
|
|
0.624 |
|
Row house |
11 |
133 |
8.3 |
|
2 |
2 |
27 |
7.4 |
|
|
Others |
5 |
70 |
7.1 |
|
3 |
25 |
263 |
9.5 |
|
|
Subtotal |
179 |
1,670 |
10.7 |
|
4 |
116 |
1,045 |
11.1 |
|
|
Thumb sucking |
|
|
|
0.024 |
5 |
24 |
250 |
9.6 |
|
|
Yes |
49 |
347 |
14.1 |
|
≥6 |
12 |
81 |
14.8 |
|
|
No |
129 |
1,320 |
9.8 |
|
Subtotal |
179 |
1,666 |
10.7 |
|
|
Subtotal |
178 |
1,667 |
10.7 |
|
Number of siblings |
|
|
|
0.346 |
|
Fingernail trimming |
|
|
|
0.036 |
1 |
30 |
315 |
9.5 |
|
|
1/week |
117 |
1,193 |
9.8 |
|
2 |
132 |
1,154 |
11.4 |
|
|
1/2weeks |
60 |
460 |
13.0 |
|
≥3 |
17 |
200 |
8.5 |
|
|
Subtotal |
177 |
1,653 |
10.7 |
|
Subtotal |
179 |
1,669 |
10.7 |
|
|
Frequency of bathing |
|
|
|
0.330 |
Recent premedication of anthelmintics |
|
|
|
0.014 |
|
1/day |
32 |
346 |
9.2 |
|
≤1 month |
0 |
66 |
0 |
|
|
2-3/week |
146 |
1,303 |
11.2 |
|
>1 months |
89 |
769 |
11.6 |
|
|
Subtotal |
178 |
1,649 |
10.8 |
|
Never |
90 |
839 |
10.7 |
|
|
Hand washing |
|
|
|
0.618 |
Subtotal |
179 |
1,674 |
10.7 |
|
|
Yes |
146 |
1,333 |
11.0 |
|
|
|
|
|
|
|
No |
32 |
327 |
9.8 |
|
|
|
|
|
|
|
Subtotal |
178 |
1,660 |
10.7 |
|
|
|
|
|
|
Table 3.Correlation of Enterobius vermicularis infection and knowledge of E. vermicularis infection
Table 3.
|
No. |
Questions |
Correct answer rate (%)
|
|
Egg positive group |
Egg negative group |
Total |
|
1 |
Stool examination is the best way to exam for Enterobius vermicularis infection. |
32.2 |
31.7 |
31.8 |
|
2 |
The adult worm of E. vermicularis migrates around the anus to mate. |
30.5 |
27.1 |
27.5 |
|
3 |
E. vermicularis enters back to the anus. Some worms can migrate to the female. genital tract so that they cause aberrant infection. |
78.0 |
80.4 |
80.1 |
|
4 |
Anal itching (pruritus ani) is one of the most common symptom of enterobiasis. |
92.1 |
93.8 |
93.6 |
|
5 |
Enterobiasis usually occurs by ingestion of eggs of contaminated hands. |
68.9 |
71.2 |
71.0 |
|
6 |
E. vermicularis infection also occurs by contact with contaminated water. |
53.7 |
51.9 |
52.1 |
|
7 |
Group therapy is the most effective for curing the E. vermicularis infection. |
67.6 |
68.1 |
68.6 |
|
8 |
E. vermicularis infection needs to repeat treatment with anthelminthic medication after 2 weeks. |
58.8 |
61.0 |
60.8 |
|
9 |
E. vermicularis infection is prevented through keeping clean and dry bedding with sunlight. |
96.0 |
93.5 |
93.7 |
|
10 |
It is crucial to practice careful hand washing and keep the nails short in preventing E. vermicularis infection. |
96.0 |
97.1 |
96.9 |
|
Average |
67.4 |
67.6 |
67.6 |
|
|
Correlation between Enterobius vermicularis infection rates and knowledge of E. vermicularis infection. |
|
Enterobius vermicularis infection* vs Knowledge of Enterobius vermicularis infection |
|
0.799 (P = 0.006) |