Abstract
Strongyloides stercoralis infection is not endemic in the Republic of Korea (Korea) with a positivity rate of <1% in stool examination. However, there is a risk of hyperinfection in immunosuppressed individuals. It is necessary to determine the seropositivity of S. stercoralis antibodies in Korea. This study investigated the seropositivity of S. stercoralis antibodies in the southeastern area of Korea. From January 2019 to June 2021, serum samples were collected from participants who visited the study center in the southeastern region of Korea for routine health check-ups. We determined serum levels of specific anti-Strongyloides IgG antibodies in 834 samples by enzyme-linked immunosorbent assay. We observed that 92 samples (11.0%) tested showed a positive response. The age of the participants was 51±10.7 years, and 43.4% of them were men. The antibody positivity rate based on the location of the participants’ residence were 12.3% (Gyoungsangnam-do), 10.2% (Busan), and 10.1% (Ulsan), respectively. Total eosinophil count was associated with positive test results (154.8±152.0 per mm3 versus 202.1±178.9 per mm3, P=0.006). Logistic regression analysis revealed that blood eosinophil count, age above 50 years, and residence in Sacheon were factors associated with the positive status of S. stercoralis antibody. Our finding suggests that it is necessary to test for S. stercoralis in actual clinical settings in Korea.
-
Key words: Strongyloides stercoralis, IgG antibody, seroprevalence, ELISA, Korea
INTRODUCTION
Strongyloides stercoralis is a parasite that causes enteric infections in animals and humans [
1]. The infection is widespread in most tropical and subtropical regions, with prevalence rate exceeding 70% in some countries, such as Peru, Dominica, Kenya, and Ghana [
2]. Moreover, the infection is distributed widely, affecting up to 370 million humans worldwide [
2]. More than 50% of cases with strongyloidiasis are asymptomatic, and the remaining cases present mainly with gastrointestinal symptoms, including abdominal pain and chronic diarrhea [
3]. However, in approximately 2.5% of cases, hyperinfection or disseminated infection that invades other organs occurs in immunocompromised patients, resulting in a serious prognosis [
4].
In the Republic of Korea (Korea), the first case of strongyloidiasis was reported in 1914, and approximately 35 cases have been reported in the literature [
3,
5–
14]. However, the seroprevalence of
S. stercoralis infection has not yet been investigated in Korea. The egg-positive rate of
S. stercoralis in stool samples was reported to be less than 1% in a previous study [
15]. The lack of serologic studies on
S. stercoralis in Korea is because clinicians did not suspect this disease, and therefore, studies for serological diagnosis of
S. stercoralis has seldom been conducted in Korea. However, a recent study reported that the prevalence of strongyloidiasis in Northeast Asia was estimated to be 5–10% [
16]. The present study aimed to investigate the seropositivity of
S. stercoralis in the southeastern area of Korea by detecting serum levels of specific anti-
Strongyloides antibodies. Further, this study analyzed the difference of epidemiologic characteristic between the seropositive and seronegative groups.
MATERIALS AND METHODS
Ethics statement
The present study had obtained ethical approval from the Institutional Review Board of Pusan National University Yangsan Hospital (approval no. 05-2021-296). Informed consent was obtained from all the participants.
Study design
This study was a retrospective cross-sectional study of a single center. In this study, samples were collected from people who visited the study center for health screening between January 2019 and June 2021. Testing for S. stercoralis antibody and data collection were performed retrospectively. The study excluded those who had a minimal serum sample volume or who refused to donate residual samples. Residual serum samples were collected from people who underwent blood tests for routine health screening. The specimens were stored by Human Material Bank of Pusan National University Yangsan Hospital. After centrifugation of the blood, the samples were stored at −40°C.
To determine the presence of IgG antibodies against
S. stercoralis, we used
Strongyloides ratti enzyme-linked immunosorbent assay (Bordier Affinity Products, Crissier, Switzerland). It has a specificity of 98.3% (95.9–100%) and a sensitivity of 89.5% (83.8–95.1%) [
17]. We used the G power 3.1.9.2 program to calculate the required sample size. More than 64 participants were needed in each positive and negative group for using independent
t test. Based on these findings, we decided to examine at least 640 specimens.
Korea has a latitude of 33° to 38° north and a longitude of 126° to 132° east. Gyeongsangnam-do (do=province), Busan, and Ulsan metropolitan city are located in the southeastern region of the Korean Peninsula. The central region has a continental dry winter climate (Dwa). By contrast, the southeastern region is a coastal region and has monsoon-influenced humid subtropical dry hot (Cwa), subtropical hot humid (Cfa), and Dwa climates (
Supplementary Figs. S1, S2) [
18]. The coastal area influences the area considerably because it is confined by high mountains to the north, which shut out the cool winter wind from the northwest. This creates the most moderate climate in Korea with an annual average temperature of 12–13°C, an annual precipitation level of 1,400–1,800 mm, and mean temperatures of −0.5°C and 25.1°C in January and August, respectively. The population in this region was 7,868,179 in 2020, accounting for 15.1% of the total population of Korea [
19,
24]. The study center was Pusan National University Yangsan Hospital, which is located in Yangsan, Gyeongsangnam-do (
Fig. 1). Owing to these regional characteristics, most of the visitors to the study center are residents of the southeastern part of Korea.
To analyze differences in age, sex, place of residence, and blood eosinophil count between the seropositive and seronegative groups, an independent t-test was used for continuous variables, and the chi-square test or Fisher’s exact test were used for categorical variables. Age was analyzed using both methods with additional categorization. For variables showing a difference in the univariate analysis, a P value of <0.05 was included in the logistic regression model. All tests were 2-sided, with a significance level of 0.05. Data analysis was performed using IBM SPSS Statistics for Windows, version 27 (IBM Corp, Armonk, New York, USA).
RESULTS
A total of 834 specimens were tested in this study, and 92 of them were seropositive (11.0%) (
Table 1). The positivity rate was significantly higher in men in the univariate analysis (
P=0.014). There were no statistically significant differences in mean age between the groups (
P=0.200). However, age >50 years was significantly associated with positive results (
P= 0.036). The eosinophil count and sex of the participants were significantly different between the positive and negative groups (
P=0.006 and
P=0.014, respectively). The positivity rate was >10% in 7 cities and rural areas, including Busan and Ulsan, which are metropolitan cities (
Table 2;
Fig. 1). In 1 city and 1 rural area, the positive rate was 50%, but the number of participants was small; therefore, caution is needed for interpretation. However, there was a statistically significant correlation between the positive test results and living in Sacheon (
P=0.020). Since this study was conducted using donated specimens, the occupation of the subjects could not be identified. Using logistic regression analysis (
Table 3), age >50 years (odds ratio (OR) =1.674, 95% confidence interval (CI): 1.049–2.672,
P=0.031), living in Sacheon City (OR=7.984, 95% CI: 1.566–40.706,
P=0.012), and blood eosinophil count (OR= 1.002, 95% CI: 1.001–1.003,
P=0.003) were found to be significantly associated with antibody test positivity. The difference in sex among the seropositive and seronegative participants was not found to be significant using the multivariate analysis (OR=1.469, 95% CI: 0.933–2.314,
P=0.096). However, it is speculated that men are more exposed to
S. stercoralis infection than women, because they tend to spend more time outdoors than women [
20]. Therefore, it is necessary to confirm whether the high antibody positive rate in male participants is an independent factor through a large-scale study in the future.
DISCUSSION
In Korea, there is a lack of studies on
S. stercoralis seropositivity. However, in recent studies, seropositivity rates of the antibody were reported to be 5–46.3% in China, Japan, and southeast Asia [
2,
16,
20–
22]. The seropositive rate of
S. stercoralis antibody in this study was 11.0%, similar to the previous study [
16].
The present study was able to confirm the following: blood eosinophil count, age >50 years, and living in Sacheon (a city located in the Gyeongsangnam-do) were significantly associated with antibody positivity. Blood eosinophil count was significantly higher in the antibody-positive group, but only 9.8% of patients in the positive group had overt eosinophilia >500 per mm
3. This finding is similar to the results of previous studies [
5,
23] and showed that blood eosinophil count should not be used as a screening test. To the best of our knowledge, this study is the first report showing serum levels of
S. stercoralis antibodies in Korea.
Notably, the positivity rate was high among the residents of Sacheon, an area where agriculture and fisheries are predominant [
19]. This city is bordered by mountains to the north and sea to the south. In addition, several small streams flow through this region. At present, it is hard to properly interpret this unexpected result. Whether geographic characteristics are related to the probability of human exposure to
S. stercoralis requires further research, including studies in populations in adjacent areas which were not included in this study.
This study included several limitations. First, the number of participants in rural areas was insufficient for analysis. Second, we could not confirm the occupations of the participants and their overseas travel history to endemic areas. Third, residents in inland areas of Korea were not included in the study. Therefore, our data may not truly represent the seropositivity rate in Korea. Fourth, because
S. stercoralis antibody test kit crossly reacted with
Toxocara canis antibody [
17], there is a possibility of some false positive cases.
Despite these limitations, our study has several implications. The antibody positivity rate is 11.0%, which suggests that there is a need for the antibody test for S. stercoralis when treating immunosuppressed patients in Korea. It would be necessary to detect specific antibody levels against S. stercoralis in actual clinical settings. Second, because Korea has regions with subtropical and continental climate, it is necessary to investigate the serological responses according to the climate. Last, the antibody positivity rate was not low, even among residents living in metropolitan cities. Investigations with a suitable study design that includes additional information, such as overseas travel history and exposure history, are required in the future.
Notes
-
The authors declare that there is no conflict of interest.
Supplementary Information
ACKNOWLEDGMENTS
The biospecimens and data used in this study were provided by the Human Material Bank of the Pusan National University Yangsan Hospital.
This study was supported by Research institute for Convergence of biomedical science and technology, Pusan National University Yangsan Hospital grant number: Incubating Task Research Support 2020.
Fig. 1Distribution of the seropositivity rate of Strongyloides stercoralis antibody in the southeastern region of Korea. Sa, Sacheon; Ch, Changnyeong; Ge, Geoje; Gi, Gimhae; Ya, Yangsan; CW, Changwon; Mi, Miryang; To, Tongyeong; HY, Hamyang.
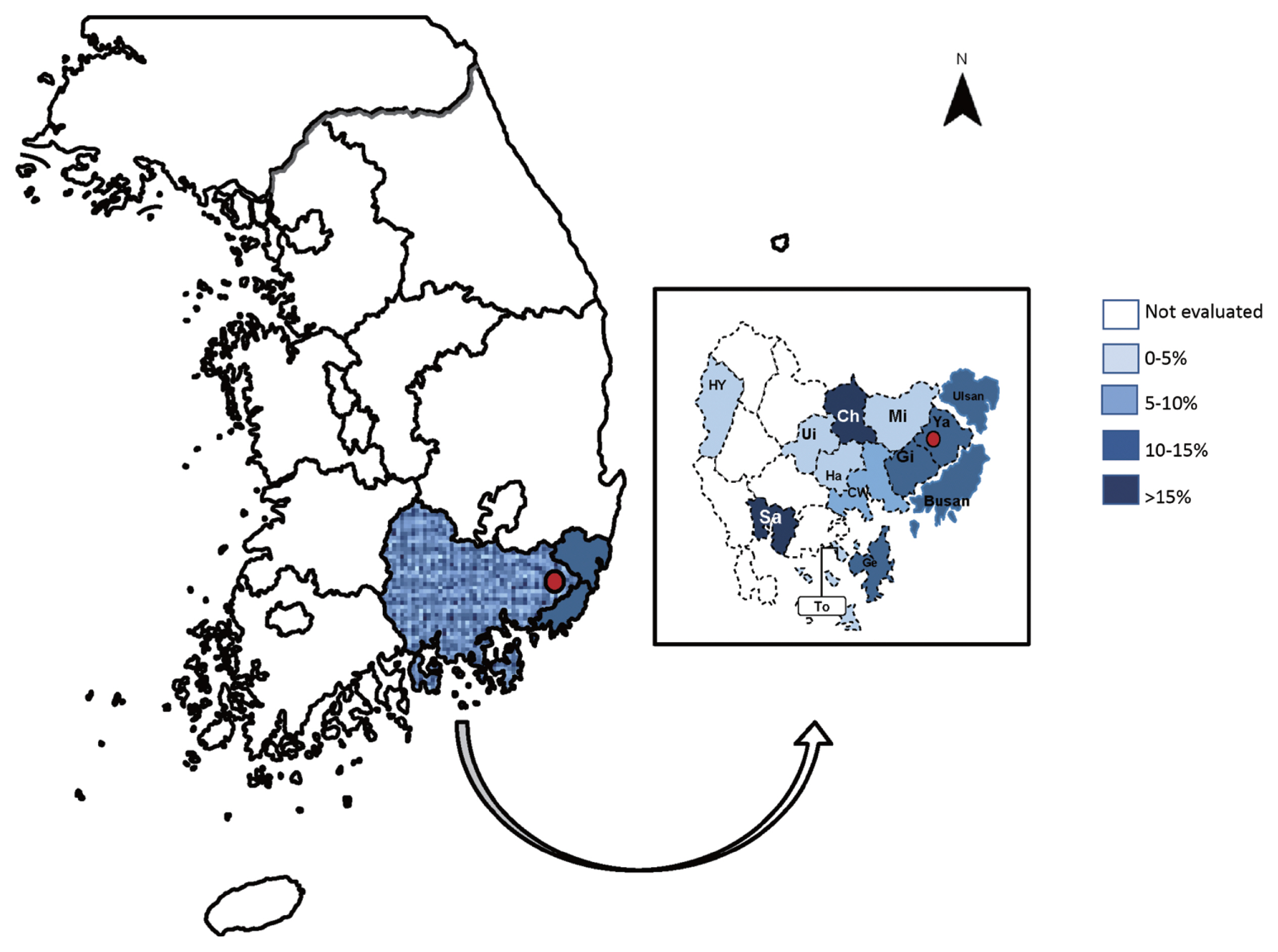
Table 1Results of Strongyloides stercoralis antibody testing according to age, sex, and eosinophil count
Table 1
|
Positive |
Negative |
Total (%) |
P-value |
|
No. (%) |
92 (11.0) |
742 (89.0) |
834 (100) |
|
|
|
Age (yr, mean±2 SD) |
52.6±10.2 |
51.0±10.8 |
51.2 (100) |
0.200 |
|
18–30 |
1 (5.9) |
16 (94.1) |
17 (2.0) |
|
|
31–40 |
14 (10.9) |
115 (89.1) |
129 (15.5) |
|
|
41–50 |
19 (8.1) |
217 (91.9) |
236 (28.3) |
|
|
51–60 |
33 (11.3) |
259 (88.7) |
292 (35.0) |
|
|
61–70 |
22 (18.0) |
100 (82.0) |
122 (14.6) |
|
|
>71 |
3 (7.9) |
35 (92.1) |
38 (4.5) |
|
|
|
Age >50 (yr) |
62 (67.4) |
415 (55.9) |
477 (57.2) |
0.036 |
|
|
Sex, Man (%) |
51 (55.4) |
311 (41.9) |
362 (43.4) |
0.014 |
|
|
Eosinophil (mean±2 SD per mm3) |
202.1±178.9 |
154.8±152.0 |
160.0±155.8 |
0.006 |
|
|
Eosinophilia (>500 per mm3) |
9 (9.8) |
26 (3.5) |
35 (4.2) |
0.010 |
Table 2Seropositive rate by administrative region in the southeastern area of Korea
Table 2
|
Administrative division |
Size of the area |
Population density (people/km2) |
Area (km2) |
Proportion of farm population (%) |
Positive No./Total (%) |
P-value |
|
Busan |
Metropolitan city |
4,349.3 |
770 |
0.8 |
33/323 (10.2) |
0.573 |
|
|
Ulsan |
Metropolitan city |
1,074.10 |
1,057 |
3.2 |
17/169 (10.1) |
0.783 |
|
|
Gyeongsangnam-do |
Province |
316.1 |
10,541 |
27.5 |
40/324 (12.3) |
0.564 |
|
Sacheon |
City |
321.7 |
398.7 |
9.5 |
3/6 (50) |
0.020 |
|
Changnyeong |
Rural area |
115.2 |
532.7 |
21.4 |
1/2 (50) |
0.209 |
|
Geoje |
City |
594.4 |
403.8 |
5.1 |
1/7 (14.3) |
0.560 |
|
Gimhae |
City |
1,170.70 |
463.4 |
3.8 |
10/71 (14.1) |
0.426 |
|
Yangsan |
City |
705.0 |
485.6 |
2.4 |
18/162 (11.1) |
1.000 |
|
Changwon |
City |
1,377.3 |
748.0 |
6.2 |
4/57 (7.0) |
0.387 |
|
Miryang |
City |
129.8 |
798.6 |
18.5 |
0/15 |
0.394 |
|
Tongyeong |
City |
520.8 |
239.8 |
5.6 |
0/2 |
1.000 |
|
Hamyang |
Rural area |
53.9 |
725.5 |
29.1 |
0/2 |
1.000 |
|
|
Other areas |
|
|
|
|
2/15 (13.3) |
0.677 |
Table 3Results of logistic regression analysis
Table 3
|
Odd ratio |
95% Confidence interval |
P-value |
|
Age above 50 years old |
1.674 |
1.049–2.672 |
0.031 |
|
Residents of Sacheon |
7.984 |
1.566–40.706 |
0.012 |
|
Eosinophil count |
1.002 |
1.001–1.003 |
0.003 |
|
Sex (Man) |
1.469 |
0.933–2.314 |
0.096 |
References
- 1. Viney ME, Lok JB. Strongyloides spp. Hodgkin J Anderson Peds, WormBook. The C. elegans Research Community; WormBook; 2007. 1-15 https://doi/10.1895/wormbook.1.141.1
- 2. Winnicki W, Eder M, Mazal P, Mayer FJ, Sengölge G, Wagner L. Prevalence of Strongyloides stercoralis infection and hyperinfection syndrome among renal allograft recipients in Central Europe. Sci Rep 2018;8:15406. https://doi.org/10.1038/s41598-018-33775-3
- 3. Park K, Kim MS, Chang J, Kim EJ, Yoo C, Kim MJ, Sung H, Kim MN. A case of chronic strongyloidiasis with recurrent hyperinfection. Lab Med Online 2019;9:171-176. (in Korean). https://doi.org/10.3343/lmo.2019.9.3.171
- 4. Keiser PB, Nutman TB. Strongyloides stercoralis in the immunocompromised population. Clin Microbiol Rev 2004;17:208-217. https://doi.org/10.1128/CMR.17.1.208-217.2004
- 5. Kim J, Joo HS, Kim DH, Lim H, Kang YH, Kim MS. A case of gastric strongyloidiasis in a Korean patient. Korean J Parasitol 2003;41:63-67. https://doi.org/10.3347/kjp.2003.41.1.63
- 6. Kim J, Joo HS, Ko HM, Na MS, Hwang SH, Im JC. A case of fatal hyperinfective strongyloidiasis with discovery of autoinfective filariform larvae in sputum. Korean J Parasitol 2005;43:51-55. https://doi.org/10.3347/kjp.2005.43.2.51
- 7. Cho JY, Kwon JG, Ha KH, Oh JY, Jin MI, Heo SW, Lee GH, Cho CH. A case of steroid-induced hyperinfective strongyloidiasis with bacterial meningitis. Korean J Gastroenterol 2012;60:330-334. (in Korean). https://doi.org/10.4166/kjg.2012.60.5.330
- 8. Rah YM, Yun SA, Yoon HJ, Lee SY. Strongyloides hyperinfection in an elderly patient treated for stomach cancer. Ann Geriatr Med Res 2014;18:241-245. (in Korean). https://doi.org/10.4235/jkgs.2014.18.4.241
- 9. Seo AN, Goo YK, Chung DI, Hong Y, Kwon O, Bae HI. Comorbid gastric adenocarcinoma and gastric and duodenal Strongyloides stercoralis infection: a case report. Korean J Parasitol 2015;53:95-99. https://doi.org/10.3347/kjp.2015.53.1.95
- 10. Won EJ, Jeon J, Koh YI, Ryang DW. Strongyloidiasis in a diabetic patient accompanied by gastrointestinal stromal tumor: cause of eosinophilia unresponsive to steroid therapy. Korean J Parasitol 2015;53:223-226. https://doi.org/10.3347/kjp.2015.53.2.223
- 11. Kim JH, Kim DS, Yoon YK, Sohn JW, Kim MJ. Donor-derived strongyloidiasis infection in solid organ transplant recipients: a review and pooled analysis. Transplant Proc 2016;48:2442-2449. https://doi.org/10.1016/j.transproceed.2015.11.045
- 12. Kim EJ. Acute respiratory distress syndrome with alveolar hemorrhage due to strongyloidiasis hyperinfection in an older patient. Ann Geriatr Med Res 2018;22:200-203. https://doi.org/10.4235/agmr.18.0041
- 13. Ra H, Chung JW, Chung DH, Kim JH, Kim YJ, Kim KO, Kwon KA, Park DK. Strongyloidiasis presenting as yellowish nodules in colonoscopy of an immunocompetent patient. Clin Endosc 2019;52:80-82. https://doi.org/10.5946/ce.2018.078
- 14. Bae J, Jeong MJ, Shin DH, Kim HW, Ahn SH, Choi JH, Yu HS. Phylogenetic positioning of a Strongyloides stercoralis isolate recovered from a Korean patient and comparison with other Asian isolates. Korean J Parasitol 2020;58:689-694. https://doi.org/10.3347/kjp.2020.58.6.689
- 15. Youn H. Review of zoonotic parasites in medical and veterinary fields in the Republic of Korea. Korean J Parasitol 2009;47:suppl. 133-141. https://10.3347/kjp.2009.47.S.S133
- 16. Buonfrate D, Bisanzio D, Giorli G, Odermatt P, Fürst T, Greenaway C, French M, Reithinger R, Gobbi F, Montresor A, Bisoffi Z. The global prevalence of Strongyloides stercoralis infection. Pathogens 2020;9:468. https://doi.org/10.3390/pathogens9060468
- 17. Bisoff Z, Buonfrate D, Sequi M, Mejia R, Cimino RO, Krolewiecki AJ, Albonico M, Gobbo M, Bonafini S, Angheben A, Requena-Mendez A. Diagnostic accuracy of five serologic tests for Strongyloides stercoralis infection. PLoS Negl Trop Dis 2014;8:e2640. https://doi.org/10.1371/journal.pntd.0002640
- 18. Beck HE, Zimmermann NE, McVicar TR, Vergopolan N, Berg A, Wood EF. Present and future Köppen-Geiger climate classification maps at 1-km resolution. Sci Data 2018;5:180214. https://doi.org/10.1038/sdata.2018.214
- 19. Statistical Geographic Information System. Population and household theme map list [Internet]; Available from: https://sgis.kostat.go.kr/view/thematicMap/thematicMapMain?stat_thema_map_id=sI&uqsnppF20160121115806975w5w92MFI5L&theme=CTGR_001&mapType=05&CTGRS=CTGR_001:recommendCTGR_002:recommend,CTGR_003:recommend,CTGR_004:recommend,CTGR_005:recommend,CTGR_006:recommend, (in Korean)
- 20. Suntaravitun P, Dokmaikaw A. Prevalence of intestinal parasites and associated risk factors for infection among rural communities of Chachoengsao Province, Thailand. Korean J Parasitol 2018;56:33-39. https://doi.org/10.3347/kjp.2018.56.1.33
- 21. Kobayashi J, Sato Y, Toma H, Shimabukuro I, Tasaki T, Takara M, Shiroma Y. Epidemiological features of strongyloides infection in Okinawa, Japan: comparative study with other endemic areas. Jpn J Trop Med Hyg 2000;28:9-14. https://doi.org/10.2149/tmh1973.28.9
- 22. Zhou X, James AA, Wang C, Li J, Chen X, Yan G, Xu J. Strongyloidiasis: an emerging infectious disease in China. Am J Trop Med Hyg 2013;88:420-425. https://doi.org/10.4269/ajtmh.12-0596
- 23. Mirzaei L, Ashrafi K, Roushan ZA, Mahmoudi MR, Masooleh IS, Rahmati B, Saadat F, Mirjalali H, Sharifdini M. Strongyloides stercoralis and other intestinal parasites in patients receiving immunosuppressive drugs in northern Iran: a closer look at risk factors. Epidemiol Health 2021;43:e2021009. https://doi.org/10.4178/epih.e2021009
- 24. Statistical Geographic Information System. Number of agricultural workers 2020 [Internet]; Available from: https://sgis.kostat.go.kr/view/thematicMap/thematicMapMain?stat_thema_map_id=JouDrDrEIF201601211158069886Mv8uqz22x&theme=CTGR_004&mapType=05&CTGRS=CTGR_001:recommendCTGR_002:recommend,CTGR_003:recommend,CTGR_004:recommend,CTGR_005:recommend,CTGR_006:recommend, (in Korean).




